Fluconazole-Darnitsa (solution for infusion)
- Capsules
- Solution for infusion
Main properties
 Release formInfusion solution
Release formInfusion solution
 ChildrenAllowed
ChildrenAllowed
 PregnantContraindicated
PregnantContraindicated NursingContraindicated
NursingContraindicated
 Release categoryPrescription medication
Release categoryPrescription medication
 Temperature storage conditionsNot higher than 25 °С
Temperature storage conditionsNot higher than 25 °С
Instructions for medical use
ЗАТВЕРДЖЕНО
Наказ Міністерства охорони здоровʼя України
13.01.2020 №48
Реєстраційне посвідчення
№ UA/14391/01/01
ІНСТРУКЦІЯ
для медичного застосування лікарського засобу
ФЛУКОНАЗОЛ-ДАРНИЦЯ
(FLUCONAZOLE-DARNITSA)
Склад:
діюча речовина: флуконазол;
1 мл розчину містить флуконазолу 2 мг;
допоміжні речовини: натрію хлорид, вода для ін’єкцій.
Лікарська форма. Розчин для інфузій.
Основні фізико-хімічні властивості: прозора безбарвна рідина.
Фармакотерапевтична група. Протигрибкові засоби для системного застосування. Похідні триазолу. Код АТХ J02A C01.
Фармакологічні властивості.
Фармакодинаміка.
Механізм дії.
Флуконазол, протигрибковий засіб класу триазолів, потужний селективний інгібітор грибкових ферментів, необхідних для синтезу ергостеролу. Первинним механізмом його дії є пригнічення грибкового 14 альфа-ланостерол-деметилювання, опосередкованого цитохромом Р450, що є невід’ємним етапом біосинтезу грибкового ергостеролу. Кумуляція 14 альфа-метил-стеролів корелює з подальшою втратою ергостеролу мембраною грибкової клітини та може відповідати за протигрибкову активність флуконазолу. Флуконазол є більш селективним до грибкових ферментів цитохрому Р450, ніж до різних систем ферментів цитохрому Р450 ссавців.
Застосування флуконазолу у дозі 50 мг на добу протягом 28 днів не впливає на рівень тестостерону у плазмі крові у чоловіків або на рівень ендогенних стероїдів у жінок репродуктивного віку. Флуконазол у дозі 200–400 мг на добу не проявляє клінічно значущого впливу на рівень ендогенних стероїдів або у відповідь на стимуляцію АКТГ у здорових добровольців чоловічої статі.
Дослідження взаємодії з антипірином продемонструвало, що застосування 50 мг флуконазолу разово або багаторазово не впливає на метаболізм антипірину.
Чутливість in vitro.
Флуконазол in vitro демонструє протигрибкову активність стосовно видів Candida, що зустрічаються найчастіше (включаючи C.albicans, C.parapsilosis, C.tropicalis). C.glabrata демонструє широкий діапазон чутливості до флуконазолу, тоді як C.krusei є до нього резистентною.
Також флуконазол in vitro демонструє активність як проти Cryptococcus neoformans та Cryptococcusgattii, так і проти ендемічних пліснявих грибів Blastomices dermatitidis, Coccidioides immitis,Histoplasma capsulatum та Paracoccidioides brasiliensis.
Фармакодинаміка–Фармакокінетика.
Відповідно до результатів досліджень на тваринах, існує кореляція між мінімальною інгібуючою концентрацією та ефективністю проти експериментальних моделей мікозів, спричинених видами Candida. Відповідно до результатів клінічних досліджень, є лінійна залежність між AUC та дозою флуконазолу (приблизно 1:1). Також є прямий, але недостатній зв’язок між AUC або дозою та позитивною клінічною відповіддю на лікування орального кандидозу та меншою мірою – кандидемії. Аналогічне лікування інфекцій, спричинених штамами, до яких флуконазол демонструє високу мінімальну інгібуючу концентрацію, є менш задовільним.
Механізм резистентності.
Мікроорганізми роду Candida демонструють чисельні механізми резистентності до азольних протигрибкових засобів. Флуконазол демонструє високу мінімальну інгібуючу концентрацію проти штамів грибів, які мають один або більше механізмів резистентності, що має негативний вплив на ефективність in vivo та в клінічній практиці. Повідомляли про випадки розвитку суперінфекції Candida spp., іншими, відмінними від C. Albicans, видами, що часто є нечутливими до флуконазолу (наприклад Candida krusei). Для лікування таких випадків слід застосовувати альтернативні протигрибкові засоби.
Фармакокінетика.
Фармакокінетичні властивості флуконазолу є подібними при внутрішньовенному і пероральному застосуванні.
Розподіл.
Об’єм розподілу приблизно дорівнює загальному вмісту рідини в організмі. Зв’язування з білками плазми крові низьке (11–12 %).
Флуконазол добре проникає в усі досліджувані рідини організму. Рівень флуконазолу у слині та мокротинні є подібним до концентрації лікарського засобу у плазмі крові. У пацієнтів, хворих на грибковий менінгіт, рівень флуконазолу у спинномозковій рідині досягає 80 % концентрації у плазмі крові.
Високі концентрації флуконазолу у шкірі, що перевищують сироваткові, досягаються у роговому шарі, епідермісі, дермі та поті. Флуконазол накопичується у роговому шарі. При застосуванні дози 50 мг 1 раз на добу концентрація флуконазолу після 12 днів лікування становила 73 мкг/г, а через 7 днів після завершення лікування концентрація все ще становила 5,8 мкг/г. При застосуванні дози 150 мг 1 раз на тиждень концентрація флуконазолу на 7-й день лікування становила 23,4 мкг/г; через 7 днів після застосування наступної дози концентрація все ще становила 7,1 мкг/г.
Концентрація флуконазолу в нігтях після 4 місяців застосування 150 мг 1 раз на тиждень становила 4,05 мкг/г у здорових добровольців та 1,8 мкг/г у пацієнтів із захворюваннями нігтів; флуконазол визначався у зразках нігтів через 6 місяців після завершення терапії.
Метаболізм.
Флуконазол метаболізується незначною мірою. При введенні дози, міченої радіоактивними ізотопами, лише 11 % флуконазолу екскретується з сечею у зміненому вигляді. Флуконазол є селективним інгібітором ізоферментів CYP2С9 та CYP3А4, а також інгібітором ізоферменту CYP2С19. Флуконазол є помірним інгібітором ізоферментів CYP2С9 та CYP3А4, а також потужним інгібітором ізоферменту CYP2С19.
Екскреція.
Період напіввиведення флуконазолу із плазми крові становить близько 30 годин. Більша частина лікарського засобу виводиться нирками, причому 80 % введеної дози виявляється у сечі в незміненому стані. Кліренс флуконазолу пропорційний до кліренсу креатиніну. Циркулюючих метаболітів не виявлено.
Тривалий період напіввиведення лікарського засобу з плазми крові дає можливість його разового застосування при вагінальному кандидозі, а також застосування препарату 1 раз на тиждень при інших показаннях.
Ниркова недостатність.
У пацієнтів із нирковою недостатністю тяжкого ступеня (швидкість клубочкової фільтрації < 20 мл/хв) період напіввиведення збільшується з 30 годин до 98 годин. Тому цій категорії пацієнтів необхідно зменшити дозу флуконазолу. Флуконазол видаляється шляхом гемодіалізу та меншою мірою – шляхом інтраперитонеального діалізу. Сеанс гемодіалізу тривалістю 3 години знижує рівень флуконазолу у плазмі крові приблизно на 50 %.
Діти.
Дані з фармакокінетики були оцінені у 113 дітей під час 5 досліджень: 2 дослідження разового застосування, 2 дослідження багаторазового застосування та 1 дослідження з участю недоношених новонароджених.
Після введення 2–8 мг/кг флуконазолу дітям віком від 9 місяців до 15 років AUC становила близько 38 мкг × годину/мл на 1 мг/кг дози. Після багаторазового застосування середній період напіввиведення флуконазолу із плазми крові варіював між 15 та 18 годинами; об’єм розподілу становив 880 мл/кг. Більш тривалий період напіввиведення із плазми крові, що становив приблизно 24 години, був після разового застосування флуконазолу. Цей показник є зіставним з періодом напіввиведення флуконазолу із плазми крові після разового застосування дози 3 мг/кг внутрішньовенно дітям віком від 11 днів до 11 місяців. Об’єм розподілу у пацієнтів цієї вікової групи становив близько 950 мл/кг.
Досвід застосування флуконазолу новонародженим обмежується фармакокінетичними дослідженнями з участю 12 недоношених дітей із терміном гестації приблизно 28 тижнів. Середній вік дитини при введенні першої дози становив 24 години (від 9 до 36 годин); середня вага при народженні становила 900 г (від 750 до 1100 г). Для 7 пацієнтів протокол дослідження було виконано. Максимум 5 внутрішньовенних ін’єкцій флуконазолу у дозі 6 мг/кг вводили кожні 72 години. Середній період напіввиведення становив 74 години (44–185) в перший день, потім зменшився до 53 годин (30–131) на 7-й день та до 47 (27–68) на 13-й день. Площа під кривою (мкг × год/мл) становила 271 (173–385) у перший день, збільшилася до 490 (292–734) на 7-й день, потім зменшилася до 360 (167–566) на 13-й день. Об’єм розподілу (мл/кг) становив 1183 (1070–1470) у перший день, збільшувався до 1184 (510–2130) на 7-й день та до 1328 (1040–1680) на 13-й день.
Пацієнти літнього віку.
Фармакокінетичне дослідження проводили з участю 22 пацієнтів (віком від 65 років), які застосовували 50 мг флуконазолу перорально. 10 учасників одночасно застосовували діуретики. Cmax становила 1,54 мкг/мл та досягалася протягом 1,3 години після застосування флуконазолу. Середня AUC становила 76,4 ± 20,3 мкг × годину/мл. Середній період напіввиведення – 46,2 години. Ці фармакокінетичні показники є вищими порівняно із аналогічними у здорових добровольців молодшого віку. Одночасне застосування діуретиків не мало значного впливу на Cmax та AUC. Також кліренс креатиніну (74 мл/хв), відсоток флуконазолу, що екскретувався із сечею у незміненому вигляді (0–24 години, 22 %) та нирковий кліренс флуконазолу (0,124 мл/хв/кг) у пацієнтів даної вікової групи були нижчими, ніж аналогічні показники у молодших добровольців. Тому зміни фармакокінетики у пацієнтів літнього віку залежать від параметрів функцій нирок.
Клінічні характеристики.
Показання.
Флуконазол-Дарниця показаний для лікування таких грибкових інфекцій у дорослих як:
– криптококовий менінгіт;
– кокцидiоїдоз;
– інвазивні кандидози;
– кандидози слизових оболонок, включаючи кандидоз ротоглотки та кандидоз стравоходу, кандидурія, хронічний кандидоз шкіри і слизових оболонок;
– хронічний атрофічний кандидоз ротової порожнини (кандидоз, спричинений використанням зубних протезів) при неефективності гігієни ротової порожнини або місцевої терапії.
Флуконазол-Дарниця показаний для профілактики таких захворювань у дорослих як:
– рецидив криптококового менінгіту у пацієнтів з високим ризиком його розвитку;
– рецидив кандидозу ротоглотки або стравоходу у пацієнтів з ВІЛ з високим ризиком його розвитку;
– профілактика кандидозних інфекцій у пацієнтів із тривалою нейтропенією (наприклад у пацієнтів зі злоякісними захворюваннями крові, які отримують хіміотерапію, чи у пацієнтів при трансплантації гемопоетичних стовбурових клітин).
Флуконазол-Дарниця застосовують дітям від народження для лікування кандидозів слизових оболонок (кандидоз ротоглотки, кандидоз стравоходу), інвазивних кандидозів, криптококового менінгіту та для профілактики кандидозних інфекцій у пацієнтів зі зниженим імунітетом. Лікарський засіб можна застосовувати як підтримуючу терапію для попередження рецидиву криптококового менінгіту у дітей із високим ризиком його розвитку.
Терапію лікарським засобом можна розпочинати до отримання результатів культуральних та інших лабораторних досліджень; після отримання результатів антибактеріальну терапію слід скоригувати відповідним чином.
Протипоказання.
Гіперчутливість до флуконазолу, до інших азольних сполук або до будь-якої з допоміжних речовин лікарського засобу.
Одночасне застосування флуконазолу та терфенадину пацієнтам, які отримують флуконазол багаторазово у дозах 400 мг/добу та вище (згідно з результатами дослідження взаємодії багаторазового застосування).
Одночасне застосування флуконазолу та інших лікарських засобів, що подовжують інтервал QT та метаболізуються за допомогою ферменту CYP3А4 (наприклад цизаприду, астемізолу, пімозиду, хінідину та еритроміцину).
Взаємодія з іншими лікарськими засобами та інші види взаємодій
Протипоказане сумісне застосування флуконазолу та нижчезазначених лікарських засобів.
Цизаприд. Повідомляли про розвиток побічних реакцій з боку серця, у тому числі про пароксизмальну шлуночкову тахікардію типу «пірует», у пацієнтів, які одночасно застосовували флуконазол та цизаприд. Контрольоване дослідження продемонструвало, що одночасне застосування 200 мг флуконазолу 1 раз на добу та 20 мг цизаприду 4 рази на добу призводило до значного підвищення рівня цизаприду у плазмі крові та до подовження інтервалу QT. Одночасне застосування флуконазолу та цизаприду протипоказане (див. розділ «Протипоказання»).
Терфенадин. Через випадки розвитку тяжких серцевих аритмій, спричинених подовженням інтервалу QTc, у пацієнтів, які застосовують азольні протигрибкові лікарські засоби одночасно з терфенадином, були проведені дослідження взаємодії цих препаратів. У ході одного дослідження при застосуванні флуконазолу у дозі 200 мг на добу не було виявлене подовження інтервалу QTc. Інше дослідження при застосуванні флуконазолу у дозах 400 та 800 мг на добу продемонструвало, що застосування флуконазолу у дозах 400 мг на добу або вище значно підвищує рівень терфенадину у плазмі крові при одночасному застосуванні цих лікарських засобів. Сумісне застосування флуконазолу у дозах 400 мг або вище з терфенадином протипоказане (див. розділ «Протипоказання»). При застосуванні флуконазолу у дозах нижче 400 мг на добу одночасно з терфенадином слід проводити ретельний моніторинг стану пацієнта.
Астемізол. Сумісне застосування флуконазолу та астемізолу може зменшити кліренс астемізолу. Спричинене цим підвищення концентрації астемізолу у плазмі крові може призвести до подовження інтервалу QT та у рідкісних випадках – до пароксизмальної шлуночкової тахікардії типу «пірует». Одночасне застосування флуконазолу та астемізолу протипоказане.
Пімозид та хінідин. Сумісне застосування флуконазолу та пімозиду або хінідину може призводити до пригнічення метаболізму пімозиду або хінідину, хоча відповідних досліджень in vitro та in vivo не проводили. Підвищення концентрації пімозиду або хінідину у плазмі крові може спричиняти подовження інтервалу QT та у рідкісних випадках призводити до розвитку пароксизмальної шлуночкової тахікардії типу «пірует». Одночасне застосування флуконазолу та пімозиду або хінідину протипоказане.
Еритроміцин. Одночасне застосування еритроміцину та флуконазолу потенційно може призводити до підвищення ризику розвитку кардіотоксичності (подовження інтервалу QT, пароксизмальна шлуночкова тахікардія типу «пірует») та, як наслідок, до раптової серцевої смерті. Застосування комбінації даних лікарських засобів протипоказане.
Не рекомендується одночасне застосування флуконазолу та нижчезазначених лікарських засобів.
Галофантрин. Флуконазол може спричинити підвищення концентрації галофантрину у плазмі крові за рахунок пригнічення CYP3A4. Одночасне застосування цих лікарських засобів може призводити до підвищення ризику розвитку кардіотоксичності (подовження інтервалу QT, пароксизмальна шлуночкова тахікардія типу «пірует») та, як наслідок, до раптової серцевої смерті. Слід уникати застосування комбінації даних лікарських засобів.
Сумісне застосування флуконазолу та нижчезазначених лікарських засобів вимагає обережності та коригування дози.
Аміодарон. Одночасне застосування флуконазолу з аміодароном може призвести до подовження інтервалу QT. Флуконазол слід з обережністю застосовувати разом з аміодароном, особливо у разі призначення високої дози флуконазолу (800 мг).
Вплив інших лікарських засобів на флуконазол.
Дослідження взаємодії продемонстрували, що пероральне застосування флуконазолу одночасно із вживанням їжі, прийомом циметидину, антацидів або з подальшим опроміненням усього тіла для пересадки кісткового мозку не має клінічно значущого впливу на абсорбцію флуконазолу.
Рифампіцин. Одночасне застосування флуконазолу та рифампіцину призводило до зниження AUC на 25 % та скорочувало період напіввиведення флуконазолу на 20 %. Тому для пацієнтів, які застосовують рифампіцин, слід розглянути доцільність підвищення дози флуконазолу.
Гідрохлоротіазид. У дослідженні фармакокінетичної взаємодії одночасне багатократне застосування гідрохлоротіазиду здоровим добровольцям, які отримували флуконазол, підвищувало концентрацію флуконазолу у плазмі крові на 40 %. Такі параметри взаємодії не вимагають змін у режимі дозування флуконазолу для пацієнтів, які одночасно отримують сечогінні засоби.
Вплив флуконазолу на інші лікарські засоби.
Флуконазол є помірним інгібітором ізоферментів CYP2C9 та CYP3A4 цитохрому P450. Флуконазол є потужним інгібітором ізоферменту CYP2С19. Окрім спостережуваних/ документально підтверджених взаємодій, що описані нижче, при одночасному застосуванні із флуконазолом існує ризик підвищення у плазмі крові концентрацій інших сполук, що метаболізуються CYP2C9, CYP2C19 та CYP3A4. Тому застосовувати такі комбінації лікарських засобів слід з обережністю; при цьому необхідно ретельно спостерігати за станом пацієнтів. Пригнічувальна дія флуконазолу на ферменти зберігається протягом 4–5 діб після його застосування у зв’язку з його тривалим періодом напіввиведення.
Аброцитиніб. Флуконазол (інгібітор CYP2C19, CYP2C9, CYP3A4) підвищував експозицію активної частини аброцитинібу на 155 %. При одночасному застосуванні з флуконазолом слід відкоригувати дозу аброцитинібу відповідно до інструкції для медичного застосування аброцитинібу.
Альфентаніл. При одночасному застосуванні альфентанілу у дозі 20 мкг/кг та флуконазолу у дозі 400 мг здоровими добровольцями спостерігалося двократне збільшення AUC10, можливо, через інгібування CYP3A4. Може бути необхідним коригування дози альфентанілу.
Амітриптилін, нортриптилін. Флуконазол посилює дію амітриптиліну та нортриптиліну.
Рекомендується вимірювати концентрації 5-нортриптиліну та/або S-амітриптиліну на початку комбінованої терапії та через 1 тиждень. У разі необхідності слід відкоригувати дозу амітриптиліну/нортриптиліну.
Амфотерицин В. Одночасне застосування флуконазолу та амфотерицину В інфікованим мишам із нормальним імунітетом та інфікованим мишам зі зниженим імунітетом призвело до таких результатів: невеликий адитивний протигрибковий ефект при системній інфекції C. albicans, відсутність взаємодії при внутрішньочерепній інфекції Cryptococcus neoformans та антагонізм двох лікарських засобів при системній інфекції A. fumigatus. Клінічне значення результатів, отриманих у ході цих досліджень, невідоме.
Антикоагулянти. Як і при застосуванні інших азольних протигрибкових засобів, при одночасному застосуванні флуконазолу та варфарину повідомляли про випадки розвитку кровотеч (гематом, носової кровотечі, шлунково-кишкових кровотеч, гематурії та мелени) у поєднанні з подовженням протромбінового часу. При одночасному застосуванні флуконазолу та варфарину спостерігалося двократне підвищення протромбінового часу, імовірно, внаслідок пригнічення метаболізму варфарину через CYP2С9. Слід ретельно контролювати протромбіновий час у пацієнтів, які одночасно застосовують кумаринові антикоагулянти або інданедіон. Може бути необхідною корекція дози антикоагулянта.
Бензодіазепіни короткої дії, наприклад мідазолам, тріазолам. Призначення флуконазолу після перорального застосування мідазоламу призводило до значного підвищення концентрації мідазоламу та до посилення психомоторних ефектів. Одночасне застосування флуконазолу у дозі 200 мг та мідазоламу у дозі 7,5 мг перорально призводило до підвищення AUC та періоду напіввиведення у 3,7 та 2,2 раза відповідно. Застосування флуконазолу у дозі 200 мг на добу та 0,25 мг тріазоламу перорально призводило до підвищення AUC та періоду напіввиведення тріазоламу 4,4 та 2,3 раза відповідно. При одночасному застосуванні флуконазолу та тріазоламу спостерігалося потенціювання та пролонгація ефектів тріазоламу.
Якщо пацієнту, який проходить курс лікування флуконазолом, слід одночасно призначити терапію бензодіазепінами, дозу останніх слід зменшити та встановити належний нагляд за станом пацієнта.
Карбамазепін. Флуконазол пригнічує метаболізм карбамазепіну та спричиняє підвищення рівня карбамазепіну в сироватці крові на 30 %. Існує ризик розвитку проявів токсичності з боку карбамазепіну. Може бути необхідним коригування дози карбамазепіну залежно від рівня його концентрації та дії лікарського засобу.
Блокатори кальцієвих каналів. Деякі антагоністи кальцію (ніфедипін, ісрадипін, амлодипін та фелодипін) метаболізуються ферментом CYP3A4. Флуконазол потенційно може підвищувати системну експозицію блокаторів кальцієвих каналів. Рекомендований ретельний моніторинг щодо розвитку побічних реакцій.
Целекоксиб. При одночасному застосуванні флуконазолу (200 мг на добу) та целекоксибу (200 мг) Cmax та AUC целекоксибу підвищувалися на 68 % та 134 % відповідно. При одночасному застосуванні целекоксибу та флуконазолу може бути необхідним зменшення дози целекоксибу вдвічі.
Циклофосфамід. Одночасне застосування циклофосфаміду та флуконазолу призводить до підвищення рівня білірубіну та креатиніну в сироватці крові. Ці лікарські засоби можна застосовувати одночасно, приділяючи особливу увагу ризику підвищення концентрації білірубіну та креатиніну в сироватці крові.
Фентаніл. Повідомляли про один летальний випадок інтоксикації фентанілом внаслідок можливої взаємодії фентанілу та флуконазолу. До того ж, у дослідженні за участю здорових добровольців було продемонстровано, що флуконазол значно уповільнював елімінацію фентанілу. Підвищення концентрації фентанілу може призвести до пригнічення дихання, тому слід ретельно контролювати стан пацієнта. Може бути необхідною корекція дози фентанілу.
Інгібітори ГМГ-КоА-редуктази. Сумісне застосування флуконазолу та інгібіторів ГМГ-КoA-редуктази, що метаболізуються CYP3A4 (аторвастатин та симвастатин), або інгібіторів ГМГ-КoA-редуктази, що метаболізуються CYP2C9 (флувастатин (зниження печінкового метаболізму статину)), підвищує ризик розвитку міопатії та рабдоміолізу (дозозалежно). У разі необхідності одночасного застосування цих лікарських засобів слід ретельно спостерігати за пацієнтом щодо виникнення симптомів міопатії та рабдоміолізу і проводити моніторинг рівня креатинкінази. У разі значного підвищення рівня креатинкінази, а також при діагностуванні або підозрі на міопатію/рабдоміоліз застосування інгібіторів ГМГ-КoA-редуктази слід припинити. Може виникнути потреба у зниженні доз інгібіторів ГМГ-КоА-редуктази, як зазначено в інструкції для медичного застосування статинів.
Ібритиніб. Помірні інгібітори CYP3A4, такі як флуконазол, підвищують концентрацію ібритинібу в плазмі та можуть підвищувати ризик токсичності. Якщо не можна уникнути комбінації препаратів, потрібно знизити дозу ібритинібу до 280 мг один раз на добу (2 капсули) з метою продовження застосування інгібітору та забезпечити постійний клінічний моніторинг.
Івакафтор (як монотерапія або в комбінації з препаратами такого самого терапевтичного класу). Одночасне застосування івакафтору, регулятора трансмембранної провідності при муковісцидозі (CFTR), збільшило експозицію івакафтору в 3 рази та експозицію гідроксиметилівакафтору (М1) у 1,9 раза. Необхідне зниження дози івакафтору (як монотерапії або в комбінації), як зазначено в інструкції для медичного застосування івакафтору (як монотерапії або в комбінації).
Олапариб. Помірні інгібітори CYP3A4, такі як флуконазол, збільшують плазмові концентрації олапарибу; їх одночасне застосування не рекомендоване. Якщо такої комбінації не можна уникнути, прийом олапарибу слід обмежувати дозами 200 мг 2 рази на добу.
Імуносупресори (наприклад, циклоспорин, еверолімус, сиролімус і такролімус).
Циклоспорин. Флуконазол значно підвищує концентрацію та AUC циклоспорину. При одночасному застосуванні флуконазолу у дозі 200 мг/добу та циклоспорину у дозі 2,7 мг/кг/добу спостерігалося збільшення AUC циклоспорину в 1,8 раза. Ці лікарські засоби можна застосовувати одночасно за умови зменшення дози циклоспорину залежно від його концентрації.
Еверолімус. Хоча досліджень in vitro та in vivo не проводили, флуконазол може підвищувати концентрацію еверолімусу в сироватці крові через пригнічення CYP3А4.
Сиролімус. Флуконазол підвищує концентрацію сиролімусу у плазмі крові, імовірно, шляхом пригнічення метаболізму сиролімусу ферментом CYP3A4 та P-глікопротеїном. Ці лікарські засоби можна застосовувати одночасно за умови коригування дози сиролімусу залежно від рівня концентрації та ефектів препарату.
Такролімус. Флуконазол може підвищувати концентрацію такролімусу в сироватці крові до 5 разів при його пероральному застосуванні через пригнічення метаболізму такролімусу ферментом CYP3A4 у кишечнику. При внутрішньовенному застосуванні такролімусу не спостерігалося значних змін фармакокінетики. Підвищені рівні такролімусу асоціюються із нефротоксичністю. Дозу такролімусу для перорального застосування слід знижувати залежно від концентрації такролімусу.
Лозартан. Флуконазол пригнічує метаболізм лозартану до його активного метаболіту (E-31 74), що зумовлює більшу частину антагонізму до рецепторів ангіотензину II під час застосування лозартану. Рекомендовано здійснювати постійний моніторинг артеріального тиску у пацієнтів.
Луразидон. Помірні інгібітори CYP3A4, такі як флуконазол, можуть підвищувати концентрацію луразидону у плазмі крові. Якщо не можна уникнути одночасного застосування, слід зменшити дозу луразидону, як зазначено в інструкції для медичного застосування луразидону.
Метадон. Флуконазол може підвищувати концентрацію метадону у сироватці крові. При одночасному застосуванні метадону та флуконазолу може бути необхідним коригування дози метадону.
Нестероїдні протизапальні препарати (НПЗП). При одночасному застосуванні з флуконазолом Cmax та AUC флурбіпрофену підвищувалися на 23 % та 81 % відповідно порівняно із такими показниками при застосуванні тільки флурбіпрофену. Аналогічно при одночасному застосуванні флуконазолу з рацемічним ібупрофеном (400 мг) Cmax та AUC фармакологічно активного ізомеру S-(+)-ібупрофену підвищувалися на 15 % та 82 % відповідно порівняно із такими показниками при застосуванні тільки рацемічного ібупрофену.
Хоча спеціальних досліджень не проводили, флуконазол потенційно здатний підвищувати системну експозицію інших НПЗП, що метаболізуються CYP2C9 (наприклад, напроксену, лорноксикаму, мелоксикаму, диклофенаку). Рекомендовано періодично здійснювати моніторинг побічних реакцій та токсичних проявів, пов’язаних із НПЗП. Може бути потрібним коригування дози НПЗП.
Фенітоїн. Флуконазол пригнічує метаболізм фенітоїну в печінці. Одночасне багаторазове застосування 200 мг флуконазолу та 250 мг фенітоїну внутрішньовенно призводить до підвищення AUC24 фенітоїну на 75 % та Сmin на 128 %. При одночасному застосуванні цих лікарських засобів слід проводити моніторинг концентрації фенітоїну у плазмі крові для уникнення розвитку токсичної дії фенітоїну.
Преднізолон. Повідомляли про випадок, коли у пацієнта після трансплантації печінки на тлі застосування преднізолону розвинулася гостра недостатність кори надниркових залоз, що виникла після припинення тримісячного курсу терапії флуконазолом. Припинення застосування флуконазолу, імовірно, спричинило посилення активності CYP3A4, що призвело до прискорення метаболізму преднізолону. Слід ретельно стежити за пацієнтами, які протягом тривалого періоду одночасно застосовують флуконазол та преднізолон, з метою попередження розвитку недостатності кори надниркових залоз після припинення застосування флуконазолу.
Рифабутин. Флуконазол підвищує концентрацію рифабутину в сироватці крові, що призводить до збільшення AUС рифабутину до 80 %. При одночасному застосуванні флуконазолу та рифабутину повідомляли про випадки розвитку увеїту. При застосуванні такої комбінації лікарських засобів слід брати до уваги симптоми токсичної дії рифабутину.
Саквінавір. Флуконазол підвищує AUC та Cmax саквінавіру приблизно на 50 % та 55 % відповідно через пригнічення метаболізму саквінавіру у печінці ферментом CYP3A4 та через інгібування P-глікопротеїну. Взаємодії між флуконазолом та саквінавіром/ритонавіром не досліджували, тому вони можуть бути більш вираженими. Може бути необхідним коригування дози саквінавіру.
Похідні сульфонілсечовини. При одночасному застосуванні флуконазол пролонгує період напіввиведення пероральних похідних сульфонілсечовини (хлорпропаміду, глібенкламіду, гліпізиду та толбутаміду) при їх застосуванні здоровим добровольцям. Рекомендується проводити частий контроль цукру в крові та відповідним чином знижувати дозу похідних сульфонілсечовини при одночасному застосуванні із флуконазолом.
Теофілін. У плацебо-контрольованому дослідженні взаємодії лікарських засобів застосування флуконазолу по 200 мг протягом 14 днів призвело до зниження середнього кліренсу теофіліну у плазмі крові на 18 %. За пацієнтами, які застосовують теофілін у високих дозах або які мають підвищений ризик розвитку токсичних проявів теофіліну з інших причин, слід встановити нагляд щодо виявлення ознак розвитку токсичної дії теофіліну. Терапію слід змінити при появі ознак токсичності.
Тофацитиніб. Вплив тофацитинібу зростає при одночасному застосуванні з лікарськими засобами, які призводять до помірного інгібування CYP3A4 та потужного інгібування CYP2C19 (наприклад, флуконазол). Тому рекомендовано зменшити дозу тофацитинібу до 5 мг 1 раз на добу в комбінаціях з цими лікарськими засобами.
Толваптан. Експозиція толваптану значно зростала (200 % AUC, 80 % Cmax), коли толваптан, субстрат CYP3A4, застосовували одночасно з флуконазолом, помірним інгібітором CYP3A4, при цьому значно зростав ризик виникнення побічних реакцій, зокрема значного збільшення діурезу, зневоднення та гострої ниркової недостатності. У разі одночасного призначення слід зменшити дозу толваптану згідно з вказівками, викладеними в інструкції для медичного застосування, та регулярно перевіряти стан пацієнта на наявність будь-яких побічних реакцій, пов’язаних із толваптаном.
Алкалоїди барвінку. Хоча відповідних досліджень не проводили, флуконазол, імовірно, через інгібування CYP3A4 може спричиняти підвищення концентрації алкалоїдів барвінку у плазмі крові (наприклад, вінкристину та вінбластину), що призводить до розвитку нейротоксичних ефектів.
Вітамін А. Повідомляли, що у пацієнта, який одночасно застосовував трансретиноєву кислоту (кислотна форма вітаміну А) та флуконазол, спостерігалися побічні реакції з боку ЦНС у формі псевдотумору головного мозку, що зник після відміни флуконазолу. Ці лікарські засоби можна застосовувати одночасно, але слід пам’ятати про ризик виникнення побічних реакцій з боку ЦНС.
Вориконазол (інгібітор CYP2С9, CYP2С19 та CYP3А4). Одночасне застосування вориконазолу перорально (по 400 мг кожні 12 годин протягом 1 дня, потім по 200 мг кожні 12 годин протягом 2,5 дня) та флуконазолу перорально (400 мг у перший день, потім по 200 мг кожні 24 години протягом 4 днів) 8 здоровим добровольцям чоловічої статі призвело до підвищення Сmax та AUCτ вориконазолу в середньому до 57 % (90 % ДІ: 20 %, 107 %) та 79 % (90 % ДІ: 40 %, 128 %) відповідно. Невідомо, чи призводить зниження дози та/або частоти застосування вориконазолу або флуконазолу до усунення такого ефекту. При застосуванні вориконазолу після флуконазолу слід проводити спостереження щодо розвитку побічних ефектів, асоційованих із вориконазолом.
Зидовудин. Флуконазол підвищує Сmax та AUC зидовудину на 84 % та 74 % відповідно, що зумовлено зниженням кліренсу зидовудину приблизно на 45 % при його пероральному застосуванні. Період напіввиведення зидовудину був також подовжений приблизно на 128 % після застосування комбінації флуконазолу та зидовудину. За пацієнтами, які застосовують таку комбінацію лікарських засобів, слід спостерігати щодо розвитку побічних реакцій, пов’язаних із застосуванням зидовудину. Можна розглянути доцільність зниження дози зидовудину.
Азитроміцин. У ході відкритого рандомізованого тристороннього перехресного дослідження, в якому взяли участь 18 здорових добровольців, оцінювали вплив азитроміцину та флуконазолу на фармакокінетику один одного при їх одночасному пероральному разовому застосуванні у дозах 1200 та 800 мг відповідно. Жодних значущих фармакокінетичних взаємодій виявлено не було.
Пероральні контрацептиви. Проводили 2 фармакокінетичних дослідження багаторазового застосування флуконазолу та комбінованого перорального контрацептива. При застосуванні флуконазолу у дозі 50 мг впливу на рівень гормонів не було, тоді як при застосуванні флуконазолу у дозі 200 мг на добу спостерігалося збільшення АUС етинілестрадіолу на 40 % та левоноргестрелу – на 24 %. Це свідчить про те, що багаторазове застосування флуконазолу у зазначених дозах навряд чи може впливати на ефективність комбінованого перорального контрацептива.
Особливості застосування.
Дерматофітія. Відповідно до результатів дослідження флуконазолу для лікування дерматофітії у дітей, флуконазол не переважає гризеофульвін за ефективністю і загальний показник ефективності становить менше 20 %. Тому лікарській засіб не слід застосовувати для лікування дерматофітії.
Криптококоз. Доказів ефективності флуконазолу для лікування криптококозу інших локалізацій (наприклад, легеневого криптококозу та криптококозу шкіри) недостатньо, тому рекомендацій щодо дозового режиму для лікування таких захворювань немає.
Глибокі ендемічні мікози. Доказів ефективності флуконазолу для лікування інших форм ендемічних мікозів, таких як паракокцидiоїдомiкоз, гістоплазмоз та шкірно-лімфатичний споротрихоз, недостатньо, тому рекомендацій щодо дозового режиму для лікування таких захворювань немає.
Ниркова система. Пацієнтам із порушенням функцій нирок лікарський засіб слід застосовувати з обережністю (див. розділ «Спосіб застосування та дози»).
Недостатність надниркових залоз. Кетоконазол, як відомо, спричиняє недостатність надниркових залоз, також може спричиняти недостатність флуконазолу, хоча таке спостерігається рідко. Недостатність надниркових залоз, пов’язана з одночасним лікуванням преднізолоном, описана в розділі «Взаємодія з іншими лікарськими засобами та інші види взаємодій. Вплив флуконазолу на інші лікарські засоби».
Гепатобіліарна система. Пацієнтам із порушенням функції печінки лікарський засіб слід застосовувати з обережністю. Застосування флуконазолу асоціювалося з виникненням рідкісних випадків розвитку тяжкої гепатотоксичності, включаючи летальні випадки, головним чином у пацієнтів із тяжкими основними захворюваннями. У разі, коли розвиток гепатотоксичності асоціювався із застосуванням флуконазолу, не було виявлено її певної залежності від загальної добової дози лікарського засобу, тривалості терапії, статі або віку пацієнта. Зазвичай гепатотоксичність, спричинена флуконазолом, оборотна, а її прояви зникають після припинення терапії.
За пацієнтами, у яких при застосуванні флуконазолу спостерігаються відхилення результатів функціональних проб печінки, слід встановити ретельний нагляд щодо розвитку більш тяжкого ураження печінки.
Пацієнтів слід проінформувати про симптоми, що можуть свідчити про серйозний вплив на печінку (виражена астенія, анорексія, постійна нудота, блювання та жовтяниця). У такому випадку застосування флуконазолу слід негайно припинити та проконсультуватися з лікарем.
Серцево-судинна система. Деякі азоли, у тому числі і флуконазол, асоціюються із подовженням інтервалу QТ на електрокардіограмі. Флуконазол подовжує інтервал QТ шляхом пригнічення випрямляючого калієвого каналу (Ikr). Подовження інтервалу QТ внаслідок дії інших лікарських засобів (наприклад аміодарону) може посилюватися шляхом пригнічення ферменту CYP3А4 цитохрому Р450. Повідомляли про дуже рідкісні випадки подовження інтервалу QТ та пароксизмальної шлуночкової тахікардії типу «пірует» при застосуванні флуконазолу. Такі повідомлення стосувалися пацієнтів із тяжкими захворюваннями при поєднанні багатьох факторів ризику, такими як структурні захворювання серця, порушення електролітного обміну та одночасне застосування інших лікарських засобів, що впливають на інтервал QТ. Пацієнти з гіпокаліємією та прогресуючою серцевою недостатністю мають підвищений ризик виникнення загрозливих для життя шлуночкових аритмій та пароксизмальної шлуночкової тахікардії типу «пірует».
Флуконазол слід з обережністю застосовувати пацієнтам із ризиком розвитку аритмій. Одночасне застосування разом із лікарськими засобами, що пролонгують інтервал QTс та метаболізуються за допомогою ферменту CYP3А4 цитохрому Р450, протипоказане.
Галофантрин. Галофантрин є субстратом ферменту CYP3А4 і пролонгує інтервал QTс при застосуванні у рекомендованих терапевтичних дозах. Одночасне застосування галофантрину та флуконазолу не рекомендується.
Дерматологічні реакції. Під час застосування флуконазолу рідко повідомляли про розвиток таких ексфоліативних шкірних реакцій як синдром Стівенса-Джонсона та токсичний епідермальний некроліз. Повідомлялося про медикаментозну реакцію з еозинофілією та системними проявами (DRESS синдром). Пацієнти зі СНІДом більш схильні до розвитку тяжких шкірних реакцій при застосуванні багатьох лікарських засобів. Якщо у пацієнта із поверхневою грибковою інфекцією з’являються висипання, що можна пов’язати із застосуванням флуконазолу, подальше застосування лікарського засобу слід припинити. Якщо у пацієнта з інвазивною/системною грибковою інфекцією з’являються висипання на шкірі, за його станом потрібно ретельно спостерігати, а у разі розвитку бульозних висипань або мультиформної еритеми застосування флуконазолу слід припинити.
Гіперчутливість. У рідкісних випадках повідомляли про розвиток анафілактичних реакцій.
Цитохром Р450. Флуконазол є помірним інгібітором ферментів CYP2C9 та CYP3А4. Також флуконазол є потужним інгібітором ферменту CYP2C19. Слід спостерігати за станом пацієнтів, які одночасно застосовують флуконазол та лікарські засоби з вузьким терапевтичним вікном, що метаболізуються з участю CYP2C9, CYP2C19 та CYP3A4.
Терфенадин. Слід ретельно спостерігати за станом пацієнта при одночасному застосуванні терфенадину та флуконазолу у дозі менше 400 мг на добу.
Кандидоз. Дослідження продемонстрували зростання поширеності інфекцій, спричинених іншими видами Candida, крім C. albicans. Вони часто є природно стійкими (наприклад C. krusei та C. auris) або демонструють знижену чутливість до флуконазолу (C. glabrata). Такі інфекції можуть потребувати альтернативної протигрибкової терапії після невдалого лікування. Отже, лікарям, які призначають засіб, рекомендується враховувати поширеність стійкості різних видів Candida до флуконазолу.
Важлива інформація про допоміжні речовини. Лікарський засіб містить 0,9 % розчин натрію хлориду. Кожні 200 мг (флакон по 100 мл) містять по 15 ммоль іонів натрію (0,145 ммоль натрію в 1 мл) та хлору, що слід брати до уваги при призначенні пацієнтам, яким необхідно обмежити вживання натрію та рідини.
Застосування у період вагітності або годування груддю.
Жінки репродуктивного віку.
Перед початком лікування пацієнтку слід проінформувати про потенційний ризик для плода.
Після застосування одноразової дози потрібно витримати період виведення флуконазолу, який становить приблизно 1 тиждень (що відповідає 5–6 періодам напіввиведення), до настання вагітності (див. підрозділ «Фармакокінетика»).
При тривалих курсах лікування жінкам репродуктивного віку слід розглянути можливість застосування контрацепції протягом усього періоду лікування та протягом 1 тижня після прийому останньої дози.
Вагітність.
Обсерваційні дослідження свідчать про підвищений ризик спонтанного аборту у жінок, які отримували флуконазол протягом першого та/або другого триместру, порівняно з жінками, які не приймали флуконазол або отримували місцеві азоли у той самий період. Дані щодо кількох тисяч вагітних жінок, які отримували лікування флуконазолом у кумулятивній дозі ≤ 150 мг у першому триместрі, демонструють відсутність зростання загального ризику вад розвитку плода. В одному великому спостережному когортному дослідженні пероральне застосування флуконазолу в першому триместрі було пов’язане з невеликим підвищенням ризику виникнення вад розвитку скелетно-м’язової системи, що відповідає приблизно 1 додатковому випадку на 1000 жінок, які отримували кумулятивні дози ≤ 450 мг, порівняно з жінками, які отримували азоли місцевої дії, і приблизно 4 додатковим випадкам на 1000 жінок, які отримували кумулятивні дози більше 450 мг. Скоригований відносний ризик становив 1,29 (95 % ДІ: 1,05–1,58) для дози флуконазолу 150 мг перорально та 1,98 (95 % ДІ: 1,23– 3,17) для доз флуконазолу більше 450 мг.
Наявні епідеміологічні дослідження щодо розвитку вад серця при застосуванні флуконазолу у період вагітності дають суперечливі результати. Однак метааналіз 5 обсерваційних досліджень, проведених за участю кількох тисяч вагітних жінок, які отримували флуконазол протягом першого триместру, виявив підвищення ризику розвитку вад серця у немовлят у 1,8–2 рази порівняно з таким у немовлят, матері яких не застосовували флуконазол та/або використовували азоли для місцевого застосування.
У повідомленнях описано вроджені вади розвитку у немовлят, матері яких отримували високі дози (від 400 до 800 мг/добу) флуконазолу у період вагітності протягом 3 місяців або більше при лікуванні кокцидіоїдомікозу. Серед вроджених вад, які спостерігалися у цих дітей, – брахіцефалія, дисплазія вушних раковин, надмірне збільшення переднього тім’ячка, викривлення стегна та променево-плечовий синостоз. Причинно-наслідковий зв’язок між застосуванням флуконазолу та вродженими вадами не встановлений.
Не слід застосовувати звичайні дози флуконазолу та короткотривалі курси лікування флуконазолом у період вагітності, за винятком нагальної потреби.
Не слід застосовувати високі дози флуконазолу та/або тривалі курси лікування флуконазолом у період вагітності, за винятком лікування інфекцій, що загрожують життю.
Період годування груддю.
Флуконазол проникає у грудне молоко та досягає нижчої концентрації, ніж у плазмі крові. Годування груддю можна продовжувати після разового застосування звичайної дози флуконазолу, що становить 150 мг.
Годувати груддю не рекомендується при багаторазовому застосуванні флуконазолу або при застосуванні його у високих доз.
Слід оцінити користь годування груддю для розвитку і здоров’я дитини, а також клінічну потребу матері у флуконазолі і будь-які потенційні побічні ефекти флуконазолу або основного захворювання матері для дитини, яка отримує грудне вигодовування.
Фертильність.
Флуконазол не впливав на фертильність самців та самок щурів.
Здатність впливати на швидкість реакції при керуванні автотранспортом або іншими механізмами.
Досліджень впливу лікарського засобу на здатність керувати автотранспортом або працювати з іншими механізмами не проводили.
Пацієнтів слід проінформувати про можливість розвитку запаморочення або судом під час застосовування лікарського засобу. При розвитку таких симптомів не рекомендується керувати автотранспортом або працювати з іншими механізмами.
Спосіб застосування та дози.
Доза флуконазолу залежить від виду і тяжкості грибкової інфекції.
При необхідності багаторазового застосування препарату лікування інфекцій слід продовжувати до зникнення клінічних та лабораторних проявів активності грибкової інфекції. Недостатня тривалість лікування може призвести до відновлення активного інфекційного процесу.
Лікарський засіб застосовувати внутрішньовенно шляхом інфузії. Немає необхідності у зміні добової дози лікарського засобу при зміні шляху його застосування з перорального на внутрішньовенний та навпаки.
Розчин для інфузій слід вводити зі швидкістю, що не перевищує 10 мл/хв.
Сумісність лікарського засобу.
Лікарський засіб сумісний з такими розчинами, як:
– 5 % та 20 % розчин глюкози;
– розчин Рінгера;
– розчин Хартмана;
– розчин калію хлориду у глюкозі;
– 4,2 % та 5 % розчин натрію бікарбонату;
– 3,5 % розчин амінозину;
– 0,9 % розчин натрію хлориду;
– діалафлекс (6,36 % розчин для інтраперитонеального діалізу).
Флуконазол можна вводити в інфузійну систему разом з одним із зазначених вище розчинів. Хоча випадки неспецифічної несумісності лікарського засобу з іншими засобами не описані, не рекомендується змішувати флуконазол з іншими лікарськими засобами перед інфузією.
Розчин для внутрішньовенних інфузій призначений лише для разового застосування. Розведення слід здійснювати в асептичних умовах. Розчин необхідно перевірити на наявність сторонніх частинок та зміну забарвлення. Розчин слід використовувати лише тоді, коли він прозорий та не містить сторонніх частинок. Невикористані залишки лікарського засобу необхідно знищити.
Дорослі.
Криптококоз.
– Лікування криптококового менінгіту: рекомендована навантажувальна доза становить 400 мг у перший день, підтримуюча доза – 200–400 мг/добу. Тривалість лікування зазвичай становить щонайменше 6–8 тижнів. При інфекціях, що загрожують життю, добову дозу можна збільшити до 800 мг.
– Підтримуюча терапія для попередження рецидиву криптококового менінгіту у пацієнтів з високим ризиком його розвитку: рекомендована доза лікарського засобу становить 200 мг/добу протягом необмеженого часу.
Кокцидiоїдоз. Рекомендована доза становить 200–400 мг/добу. Тривалість лікування – 11–24 місяці чи довше залежно від стану пацієнта. Для лікування деяких форм інфекції, а особливо для лікування менінгіту може бути доцільним застосування дози 800 мг/добу.
Інвазивні кандидози. Навантажувальна доза становить 800 мг у перший день, підтримуюча доза – 400 мг/добу. Зазвичай рекомендована тривалість лікування кандидемії становить 2 тижні після перших негативних результатів культури крові та зникнення ознак і симптомів кандидемії.
Кандидоз слизових оболонок.
– Кандидоз ротоглотки: навантажувальна доза становить 200–400 мг у перший день, підтримуюча доза – 100–200 мг/добу. Тривалість лікування становить 7–21 день (до досягнення ремісії), але може бути збільшена для пацієнтів із тяжким імунодефіцитом.
– Кандидоз стравоходу: навантажувальна доза становить 200–400 мг у перший день, підтримуюча доза – 100–200 мг/добу. Тривалість лікування становить 14–30 днів (до досягнення ремісії), але може бути збільшена для пацієнтів із тяжким імунодефіцитом.
– Кандидурія: рекомендована доза становить 200–400 мг/добу протягом 7–21 дня. Для пацієнтів із тяжким імунодефіцитом тривалість лікування можна збільшити.
– Хронічний атрофічний кандидоз: рекомендована доза становить 50 мг/добу протягом 14 днів.
– Хронічний кандидоз шкіри та слизових оболонок: рекомендована доза становить 50–100 мг/добу. Тривалість лікування – до 28 днів, але може бути збільшена залежно від тяжкості та виду інфекції або зниження імунітету.
Попередження рецидиву кандидозу слизових оболонок у пацієнтів з ВІЛ, які мають високий ризик його розвитку.
– Кандидоз ротоглотки, кандидоз стравоходу: рекомендована доза становить 100–200 мг/добу або 200 мг 3 рази на тиждень. Тривалість лікування є необмеженою для пацієнтів із пригніченим імунітетом.
Профілактика кандидозних інфекцій у пацієнтів із тривалою нейтропенією. Рекомендована доза становить 200–400 мг. Лікування слід розпочинати за кілька днів до очікуваного розвитку нейтропенії та продовжувати протягом 7 днів після підвищення кількості нейтрофілів понад 1000/мм3.
Пацієнти літнього віку.
Дозу необхідно підбирати залежно від стану функції нирок (див. нижче).
Пацієнти з нирковою недостатністю.
Флуконазол виводиться з організму переважно з сечею у незміненому вигляді. При разовому застосуванні коригувати дозу не потрібно. Пацієнтам (включаючи дітей) із порушенням функцій нирок при необхідності багаторазового застосування препарату у перший день лікування слід застосовувати початкову дозу 50–400 мг залежно від показань. Після цього добову дозу (залежно від показань) слід розраховувати відповідно до таблиці:
Кліренс креатиніну (мл/хв) | Відсоток від рекомендованої дози |
> 50 | 100 % |
≤ 50 (без гемодіалізу) | 50 % |
Гемодіаліз | 100 % після кожного гемодіалізу |
Пацієнти, які перебувають на гемодіалізі, повинні отримувати 100 % рекомендованої дози після кожного гемодіалізу. У день, коли діаліз не проводиться, пацієнт повинен отримувати дозу, відкориговану залежно від кліренсу креатиніну.
Пацієнти з порушенням функції печінки.
Флуконазол слід застосовувати з обережністю пацієнтам із порушеннями функції печінки, оскільки інформації щодо застосування флуконазолу цій категорії пацієнтів недостатньо.
Діти.
Не слід перевищувати максимальну добову дозу 400 мг.
Як і при аналогічних інфекціях у дорослих, тривалість лікування залежить від клінічної та мікологічної відповіді. Флуконазол застосовувати 1 раз на добу.
Дозування лікарського засобу дітям із порушенням функції нирок наведено у підрозділі «Пацієнти з нирковою недостатністю».
Фармакокінетика флуконазолу не досліджувалася у дітей із нирковою недостатністю (див. нижче інформацію щодо застосування новонародженим, у яких часто спостерігається первинна незрілість нирок).
Діти віком від 12 років.
Залежно від маси тіла та пубертатного розвитку лікарю слід оцінити, яка доза лікарського засобу (для дорослих або для дітей) є оптимальною для пацієнта. Клінічні дані свідчать про те, що у дітей кліренс флуконазолу є вищим порівняно з дорослими. Застосування доз 100, 200 та 400 мг дорослим та доз 3, 6 та 12 мг/кг дітям призводить до досягнення зіставної системної експозиції.
Діти віком від 28 днів до 11 років.
- Кандидози слизових оболонок: початкова доза становить 6 мг/кг/добу, підтримуюча доза –3 мг/кг/добу. Початкову дозу можна застосовувати в перший день з метою більш швидкого досягнення рівноважної концентрації.
- Інвазивні кандидози, криптококовий менінгіт: доза лікарського засобу становить 6–12 мг/кг/добу залежно від ступеня тяжкості захворювання.
- Підтримуюча терапія для попередження рецидиву криптококового менінгіту у дітей із високим ризиком його розвитку: доза лікарського засобу становить 6 мг/кг/добу залежно від ступеня тяжкості захворювання.
- Профілактика кандидозів у пацієнтів з імунодефіцитом: доза лікарського засобу становить 3–12 мг/кг/добу залежно від вираженості та тривалості індукованої нейтропенії (див. дози для дорослих).
Діти віком від народження до 27 днів.
У новонароджених флуконазол виводиться з організму повільно. Дані з фармакокінетики, на яких базуються дози для доношених новонароджених, зазначені нижче, наведено в розділі «Фармакокінетика».
– Доношені новонароджені віком від 0 до 14 днів: дози, аналогічні зазначеним вище для дітей віком від 28 днів до 11 років, слід застосовувати кожні 72 години. Не слід перевищувати максимальну дозу, що становить 12 мг/кг кожні 72 години.
– Доношені новонароджені віком від 15 до 27 днів: дози, аналогічні зазначеним вище для дітей віком від 28 днів до 11 років, слід застосовувати кожні 48 годин. Не слід перевищувати максимальну дозу, що становить 12 мг/кг кожні 48 годин.
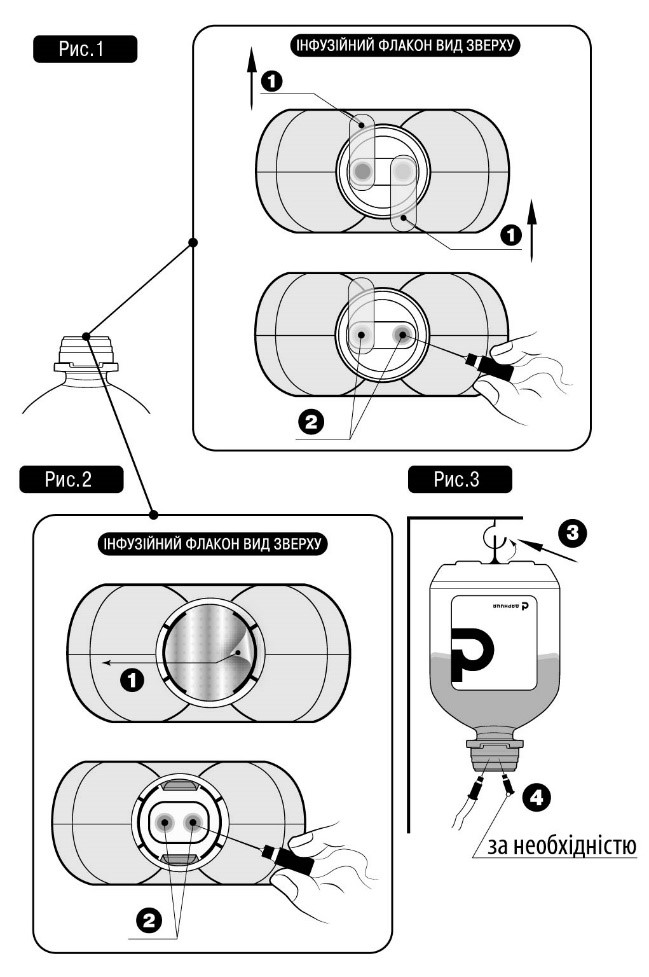
Спосіб застосування
Не вставляти голку(-и) у не передбачені для цього місця полімерного флакона, а тільки у стерильні порти!
Для проведення інфузійного лікування потрібно дотримуватись такого алгоритму:
Зняти захисну пластикову кришку із контролем першого відкриття (якщо така наявна).
Зірвати захисний(-і) клапан(-и) № 1, як показано на рис. 1 та рис.2 (виробник може використовувати різні типи та матеріали для захисних клапанів).
Зняти ковпачок із голки та вставити у будь-який зі спеціальних портів № 2 флакона з інфузійним лікарським засобом (див. рис. 1 та рис. 2).
Інший стерильний порт може використовуватись для введення в інфузійний флакон інших лікарських засобів (№ 4, див. рис. 3), або, у разі недостатньої швидкості потоку для голки-повітровода (№ 4, див. рис. 3).
Підвісити флакон із розчином, використовуючи спеціальне кільце № 3, розташоване на дні флакона (див. рис. 3).
Діти. Лікарський засіб можна застосовувати дітям від народження, див. розділ «Спосіб застосування та дози».
Передозування.
Отримано повідомлення про передозування флуконазолом; одночасно повідомляли про галюцинації та параноїдальну поведінку.
При передозуванні потрібно провести симптоматичну підтримуючу терапію та у разі необхідності промити шлунок.
Флуконазол значною мірою екскретується з сечею; форсований діурез може прискорити виведення лікарського засобу. Сеанс гемодіалізу тривалістю 3 години знижує рівень флуконазолу у плазмі крові приблизно на 50 %.
Побічні реакції.
Найчастіше (> 1/10) повідомляли про такі побічні реакції: головний біль, абдомінальний біль, діарея, нудота, блювання, висипання, підвищення рівня аланінамінотрансферази (АЛТ), аспартатамінотрансферази (АСТ) та лужної фосфатази крові, реакція на лікарський засіб, що супроводжується еозинофілією та системними проявами (DRESS-синдром), що пов’язана з лікуванням флуконазолом (див. розділ «Особливості застосування»).
Для оцінки частоти виникнення побічних реакцій використовують таку класифікацію: дуже часто (≥ 1/10), часто (від ≥ 1/100 до < 1/10), нечасто (від ≥ 1/1000 до < 1/100), рідко (від ≥ 1/10000 до < 1/1000), дуже рідко (< 1/10000), частота невідома (неможливо оцінити на підставі наявних даних).
З боку органів слуху та вестибулярного апарату:
Нечасто: вертиго.
З боку шлунково-кишкового тракту:
Часто: біль у черевній порожнині, нудота, діарея, блювання.
Нечасто: запор, диспепсія, метеоризм, сухість у роті.
З боку печінки і жовчовивідних шляхів:
Часто: підвищення рівня аланінамінотрансферази (АЛТ), підвищення рівня аспартатамінотрансферази (АСТ), підвищення рівня лужної фосфатази.
Нечасто: холестаз, жовтяниця, підвищення рівня білірубіну.
Рідко: печінкова недостатність, гепатоцелюлярний некроз, гепатити, гепатоцелюлярне ураження.
З боку обміну речовин, метаболізму:
Нечасто: зниження апетиту.
Рідко: гіперхолестеринемія, гіпертригліцеридемія, гіпокаліємія.
З боку нервової системи:
Часто: головний біль.
Нечасто: судоми, парестезія, запаморочення, порушення смаку.
Рідко: тремор.
З боку психіки:
Нечасто: безсоння, сонливість.
З боку серцево-судинної системи:
Рідко: пароксизмальна шлуночкова тахікардія типу «пірует», подовження інтервалу QT.
З боку крові та лімфатичної системи:
Нечасто: анемія.
Рідко: агранулоцитоз, лейкопенія, тромбоцитопенія, нейтропенія.
З боку імунної системи:
Рідко: анафілаксія.
З боку шкіри та підшкірної клітковини:
Часто: висипання.
Нечасто: медикаментозний дерматит (включаючи фіксований медикаментозний дерматит), кропив’янка, свербіж, підвищене потовиділення.
Рідко: токсичний епідермальний некроліз, синдром Стівенса-Джонсона, гострий генералізований екзантематозний пустульоз, ексфоліативний дерматит, ангіоневротичний набряк, набряк обличчя, алопеція.
Невідомо: реакція на лікарський засіб з еозинофілією та системними симптомами (DRESS).
З боку опорно-рухової системи та сполучної тканини:
Нечасто: міалгія.
Загальні розлади та реакції у місці введення:
Нечасто: підвищена втомлюваність, нездужання, астенія, гарячка.
Діти. Частота та характер побічних реакцій і відхилень від норми результатів лабораторних аналізів у ході клінічних досліджень з участю дітей зіставні з такими у дорослих.
Повідомлення про підозрювані побічні реакції.
Повідомлення про підозрювані побічні реакції після реєстрації лікарського засобу є важливою процедурою. Це дозволяє продовжувати моніторинг співвідношення «користь/ризик» для відповідного лікарського засобу. Медичним працівникам необхідно повідомляти про будь-які підозрювані побічні реакції через національну систему повідомлень.
Термін придатності. 3 роки.
Умови зберігання.
Зберігати в оригінальній упаковці при температурі не вище 25 °С. Не заморожувати.
Зберігати у недоступному для дітей місці.
Несумісність.
Особливостей щодо несумісності лікарського засобу не відзначено. Не слід змішувати препарат з іншими лікарськими засобами в одній ємкості, окрім зазначених у розділі «Спосіб застосування та дози».
Упаковка.
По 100 мл у флаконі; по 1 флакону в пачці; по 100 мл у флаконах.
Категорія відпуску. За рецептом.
Виробник. ПрАТ «Фармацевтична фірма «Дарниця».
Місцезнаходження виробника та адреса місця провадження його діяльності.
Україна, 02093, м. Київ, вул. Бориспiльська, 13.
Дата останнього перегляду. 03.06.2025