Leflock-Darnitsa
Antibacterial agents of the quinolone group. Fluoroquinolones- Solution for infusion
- Film-coated tablets
Main properties
 Release formInfusion solution
Release formInfusion solution
 ChildrenContraindicated
ChildrenContraindicated PregnantContraindicated
PregnantContraindicated NursingContraindicated
NursingContraindicated
 Release categoryPrescription medication
Release categoryPrescription medication
 AllergicsWith caution
AllergicsWith caution DiabeticsWith caution
DiabeticsWith caution With alcoholContraindicated
With alcoholContraindicated DriversWith caution
DriversWith caution
 Temperature storage conditionsNot higher than 25 °С
Temperature storage conditionsNot higher than 25 °С
Instructions for medical use
ЗАТВЕРДЖЕНО
Наказ Міністерства охорони здоровʼя України
02.10.2019 № 2004
Реєстраційне посвідчення
№ UA/14011/01/01
ІНСТРУКЦІЯ
для медичного застосування лікарського засобу
ЛЕФЛОК-ДАРНИЦЯ (LEFLOCK-DARNITSA)
діюча речовина: levofloxacin;
1 мл розчину містить левофлоксацину гемігідрату в перерахуванні на левофлоксацин 5 мг;
допоміжні речовини: натрію хлорид, кислота хлористоводнева розведена, натрію гідроксид, вода для ін’єкцій.
Лікарська форма. Розчин для інфузій.
Основні фізико-хімічні властивості: прозора рідина від жовтого до жовтого із зеленуватим відтінком кольору.
Фармакотерапевтична група.
Антибактеріальні засоби групи хінолонів. Фторхінолони. Код АТХ J01M А12.
Фармакологічні властивості.
Фармакодинаміка.
Левофлоксацин – синтетичний антибактеріальний засіб із групи фторхінолонів, S-енантіомер рацемічної суміші лікарського засобу офлоксацину. Як антибактеріальний лікарський засіб із групи фторхінолонів, левофлоксацин діє на комплекс ДНК з ДНК-гірази та топоізомерази ІV. Основний механізм резистентності є наслідком мутації у генах gyr-A.
In vitro існує перехресна резистентність між левофлоксацином та іншими фторхінолонами.
Межові значення.
Рекомендовані Європейським комітетом із тестування антимікробної чутливості (EUCAST) межові значення МІК для левофлоксацину, що відділяють чутливі мікроорганізми від організмів проміжно чутливих (помірно резистентних) та проміжно чутливі від резистентних організмів, представлені в Таблиці 1 тестування МІК (мг/л).
Клінічні межові значення МІК EUCAST для левофлоксацину:
Таблиця 1
Патогени | Чутливі | Резистентні |
| Enterobacteriacae | ≤ 1 мг/л | > 2 мг/л |
| Pseudomonas spp. | ≤ 1 мг/л | > 2 мг/л |
| Acinetobacter spp. | ≤ 1 мг/л | > 2 мг/л |
| Staphylococcus spp. | ≤ 1 мг/л | > 2 мг/л |
| S. pneumoniae 1 | ≤ 2 мг/л | > 2 мг/л |
| Streptococcus A, B, C, G | ≤ 1 мг/л | > 2 мг/л |
| H. influenzae 2, 3 | ≤ 1 мг/л | > 1 мг/л |
| M. catarrhalis 3 | > 1 мг/л | > 1 мг/л |
| Межові значення, не пов’язані з видами 4 | ≤ 1 мг/л | > 2 мг/л |
1 Межові значення левофлоксацину стосуються терапії високих доз.
2 Можливий низький рівень резистентності до фторхінолонів (МІК ципрофлоксацину 0,12−0,5 мг/л), але не існує доказів того, що така резистентність має клінічне значення при інфекціях дихальних шляхів, спричинених H. influenzae.
3 Штами з величинами МІК, вищими від межового значення між чутливими та проміжно чутливими (помірно резистентними) штамами, є дуже рідкісними або про них ще не повідомляли. Тести на ідентифікацію та протимікробну чутливість на будь-якому такому ізоляті слід повторити і, якщо результат буде підтверджено, надіслати ізолят до уповноваженої лабораторії. Поки є дані, що свідчать про клінічну реакцію для підтверджених ізолятів з МІК вище поточного резистентного межового значення, про них необхідно повідомляти як про резистентні.
4 Межові значення пероральних доз від 500 мг одноразово до 500 мг х 2 рази на добу і внутрішньовенних доз від 500 мг одноразово до 500 мг х 2 рази на добу.
Антибактеріальний спектр
Поширеність резистентності для вибраних видів може варіювати географічно та з часом. Бажано отримати місцеву інформацію про резистентність, особливо при лікуванні тяжких інфекцій.
Зазвичай чутливі види.
Аеробні грампозитивні бактерії: Bacillus anthracis, Staphylococcus aureus* метицилінчутливий, Staphylococcus saprophyticus, Streptococci − група С і G, Streptococcus agalactiae, Streptococcus pneumoniae*, Streptococcus pyogenes*.
Аеробні грамнегативні бактерії: Burkholderia cepacia**, Eikenella corrodens, Haemophilus influenzae*, Haemophilus para-influenzae*, Klebsiella oxytoca, Moraxella catarrhalis*, Pasteurella multocida, Proteus vulgaris, Providencia rettgeri.
Анаеробні бактерії: Peptostreptococcus.
Інші: Chlamydophila pneumoniae*, Chlamydophila psittaci, Chlamidia trachomatis, Legionella pneumophila*, Mycoplasma pneumoniae*, Mycoplasma hominis, Ureaplasma urealyticum.
Види, набута (вторинна) резистентність яких може становити проблему.
Аеробні грампозитивні бактерії: Enterococcus faecalis*, Staphylococcus aureus метицилін-резистентний, Staphylococcus coagulase spp.
Аеробні грамнегативні бактерії: Acinetobacter baumannii*, Citrobacter freundii*, Enterobacter aerogenes, Enterobacter agglomerans, Enterobacter cloacae*, Escherichia coli*, Klebsiella pneumoniae, Morganella morganii*, Proteus mirabilis*, Providencia stuartii, Pseudomonas aeruginosa*, Serratia marcescens*.
Анаеробні бактерії: Bacteroides fragilis, Bacteroides ovatus**, Bacteroides thetaiotamicron**, Bacteroides vulgatus**, Clostridium difficile**.
Природно резистентні штами.
Аеробні грампозитивні бактерії: Enterococcus faecium.
* Клінічна ефективність була продемонстрована для чутливих ізолятів у затверджених клінічних показаннях.
** Природна помірна чутливість.
Інші дані.
Госпітальні інфекції, викликані Pseudomonas aeruginosa, можуть потребувати комбінованої терапії.
Фармакокінетика.
Абсорбція
Немає суттєвої різниці у фармакокінетиці левофлоксацину після внутрішньовенного та перорального застосування. Після внутрішньовенного введення лікарський засіб накопичується у слизовій оболонці бронхів та бронхіальному секреті тканини легенів (концентрація у легенях перевищує таку у плазмі крові), у сечі. У спинномозкову рідину левофлоксацин потрапляє погано.
Розподіл
Приблизно 30−40 % левофлоксацину зв’язується з протеїном сироватки крові. Кумуляційний ефект від багаторазового застосування левофлоксацину у дозі 500 мг 1 раз на добу практично відсутній. Існує незначний, але передбачуваний кумуляційний ефект після застосування доз по 500 мг 2 рази на добу. Стабільний стан досягається протягом 3 днів.
Проникнення у тканини та рідини організму
Проникнення у слизову оболонку бронхів, бронхіальний секрет тканин легенів
Максимальна концентрація левофлоксацину у слизовій оболонці бронхів та бронхіальному секреті легенів після застосування 500 мг перорально становила 8,3 та 10,8 мкг/мл відповідно. Ці показники досягалися протягом 1 години після прийому лікарського засобу.
Проникнення у тканини легенів
Максимальна концентрація левофлоксацину у тканинах легенів після застосування 500 мг перорально становила приблизно 11,3 мкг/г та досягалася через 4−6 годин після застосування лікарського засобу. Концентрація у легенях перевищує таку у плазмі крові.
Проникнення у вміст пухирів (шкіра)
Максимальна концентрація левофлоксацину (4,0−6,7 мкг/мл) у вмісті пухира досягалася через 2−4 години після введення лікарського засобу протягом 3 днів застосування у дозах 500 мг 1 або 2 рази на добу відповідно.
Проникнення у цереброспінальну (спинномозкову) рідину
Левофлоксацин погано проникає у цереброспінальну рідину.
Проникнення у тканини простати
Після застосування 500 мг левофлоксацину 1 раз на добу протягом 3 днів середні концентрації у тканині простати досягали 8,7 мкг/г, 8,2 мкг/г та 2 мкг/г відповідно через 2 години, 6 годин та 24 години; середній коефіцієнт концентрації простата/плазма становив 1,84.
Концентрація у сечі
Середня концентрація у сечі через 8−12 годин після одноразового прийому перорально дози 150 мг, 300 мг та 500 мг левофлоксацину становила 44 мг/л, 91 мг/л та 200 мг/л відповідно.
Біотрансформація
Левофлоксацин метаболізується незначною мірою, метаболітами є дисметил-левофлоксацин та левофлоксацину N-оксид. Ці метаболіти становлять менше 5 % кількості лікарського засобу, що виділяється із сечею. Левофлоксацин є стереохімічно стабільним та не підлягає інверсії хоральної структури.
Виведення
Після перорального та внутрішньовенного введення левофлоксацин виводиться з плазми крові відносно повільно (період напіввиведення становить 6−8 годин). Виводиться в основному нирками (понад 85 % введеної дози).
Немає суттєвої різниці у фармакокінетиці левофлоксацину після внутрішньовенного та перорального введення, що свідчить про те, що ці шляхи введення є взаємозамінними.
Лінійність
Левофлоксацин має лінійну фармакокінетику у діапазоні 50−600 мг.
Пацієнти з нирковою недостатністю
На фармакокінетику левофлоксацину впливає ниркова недостатність. При зниженні функції нирок знижується ниркове виведення та кліренс, а період напіввиведення збільшується, як видно з Таблиці 2.
Таблиця 2
Кліренс креатиніну (мл/хв) | < 20 | 20−49 | 50−80 |
Нирковий кліренс (мл/хв) | 13 | 26 | 57 |
Період напіввиведення (год) | 35 | 27 | 9 |
Пацієнти літнього віку
Немає значних відмінностей у фармакокінетиці левофлоксацину у молодих пацієнтів та пацієнтів літнього віку, крім відмінностей, пов’язаних із кліренсом креатиніну.
Гендерні відмінності
Окремий аналіз груп пацієнтів жіночої та чоловічої статі продемонстрував незначні відмінності у фармакокінетиці левофлоксацину залежно від статі. Не існує доказів того, що ці гендерні відмінності у фармакокінетиці є клінічно значущими.
Клінічні характеристики.
Показання.
Лефлок, розчин для інфузій, призначають дорослим для лікування таких інфекційних захворювань, спричинених чутливими до левофлоксацину мікроорганізмами:
− негоспітальна пневмонія*;
− ускладнені інфекції шкіри та м’яких тканин*;
− гострий пієлонефрит та ускладнені інфекції сечовивідних шляхів;
− хронічний бактеріальний простатит;
− легенева форма сибірської виразки: постконтактна профілактика та радикальне лікування.
*стосовно вищевказаних інфекційних захворювань левофлоксацин слід призначати лише у випадках недостатньої ефективності інших антибактеріальних лікарських засобів, які переважно застосовують для початкового лікування даних інфекцій.
Слід враховувати офіційні рекомендації щодо належного застосування антибактеріальних засобів.
Протипоказання.
− Підвищена чутливість до левофлоксацину, інших хінолонів, до будь-якого компонента лікарського засобу.
− Побічні реакції з боку сухожиль після попереднього застосування хінолонів.
− Епілепсія.
− Дитячий вік (до 18 років).
− Період вагітності або годування груддю.
Взаємодія з іншими лікарськими засобами та інші види взаємодій.
Tеофілін, фенбуфен або подібні нестероїдні протизапальні препарати (НПЗП)
Можливе суттєве зниження судомного порогу при одночасному застосуванні хінолонів з теофіліном, НПЗП та іншими речовинами, що знижують судомний поріг. Концентрація левофлоксацину при наявності фенбуфену приблизно на 13 % вища, ніж при прийомі лише левофлоксацину.
Пробенецид і циметидин
Пробенецид і циметидин статистично достовірно впливають на виведення левофлоксацину. Нирковий кліренс левофлоксацину знижується при наявності пробенециду на 34 %, а циметидину – на 24 %. Через це обидва препарати здатні блокувати канальцеву екскрецію левофлоксацину. Їх слід з обережністю застосовувати пацієнтам із нирковою недостатністю.
Циклоспорин
Період напіввиведення циклоспорину збільшується на 33 % при введенні його одночасно з левофлоксацином.
Антагоністи вітаміну К
При одночасному застосуванні з антагоністами вітаміну К (наприклад, із варфарином) підвищуються значення коагуляційних тестів (ПЧ/міжнародне нормалізаційне співвідношення). Можливі виражені кровотечі. Зважаючи на це, у пацієнтів, які одержують паралельно антагоністи вітаміну К, необхідно здійснювати контроль показників коагуляції.
Лікарські засоби, що подовжують інтервал QT
Левофлоксацин, як і інші фторхінолони, слід з обережністю застосовувати пацієнтам, які отримують лікарські засоби, що подовжують інтервал QT (зокрема антиаритмічні засоби класів ІА і ІІІ, трициклічні антидепресанти, макроліди, антипсихотичні лікарські засоби).
Теофілін
Левофлоксацин не впливає на фармакокінетику теофіліну, який переважно метаболізується з допомогою CYP1A2, тому можна вважати, що левофлоксацин не є інгібітором CYP1A2.
Глюкокортикоїди
При одночасному застосуванні з глюкокортикоїдами підвищується ризик розвитку розриву сухожилля.
Інше
Не спостерігалося ніякого клінічно значущого впливу на фармакокінетику левофлоксацину при його застосуванні разом з такими лікарськими засобами: карбонатом кальцію, дигоксином, глібенкламідом, ранітидином.
Не рекомендується застосування левофлоксацину одночасно з алкоголем.
Особливості застосування.
Слід уникати застосування лікарського засобу пацієнтам, які мали серйозні побічні реакції в минулому при застосуванні хінолонів або фторхінолонів. Лікування цих пацієнтів левофлоксацином слід починати тільки за відсутності альтернативних варіантів лікування і після ретельної оцінки користі/ризику.
Тривалі, інвалідизуючі і потенційно незворотні серйозні побічні реакції
У дуже рідкісних випадках у пацієнтів, які отримували фторхінолони, незалежно від віку та наявних факторів ризику повідомляли про тривалі (протягом місяців або років) інвалідизуючі та потенційно незворотні серйозні побічні реакції, які впливають на різні, а іноді на декілька відразу, системи організму (опорно-рухову, нервову, психіку та органи чуття). Застосування лікарського засобу слід негайно припинити після появи перших ознак або симптомів будь-якої серйозної побічної реакції та слід звернутися за консультацією до лікаря.
Хворим із вираженими порушеннями функції нирок, а також із вираженим атеросклерозом судин головного мозку, порушеннями мозкового кровообігу слід бути обережними при застосуванні лікарського засобу.
Протягом усього курсу лікування необхідно контролювати функцію нирок і печінки.
При застосуванні лікарського засобу слід утримуватися від вживання алкоголю.
При дуже тяжкому перебігу запалення легенів, спричиненому пневмококами, левофлоксацин може не дати оптимального терапевтичного ефекту.
Госпітальні інфекції, спричинені Pseudomonas aeruginosa, можуть потребувати комбінованої терапії.
Тривалість введення
Рекомендована тривалість введення лікарського засобу становить щонайменше 60 хвилин для 500 мг розчину для інфузій. Стосовно офлоксацину відомо, що під час інфузії можуть відзначатися тахікардія та тимчасове підвищення артеріального тиску. У рідкісних випадках може спостерігатися раптове зниження артеріального тиску, циркуляторний колапс. Якщо під час введення левофлоксацину спостерігається виражене зниження артеріального тиску, введення слід негайно припинити.
Аневризма і розшарування аорти
Епідеміологічні дослідження свідчать про підвищений ризик аневризми та розшарування аорти після застосування фторхінолонів, особливо у літніх людей.
Тому фторхінолони слід застосовувати тільки після ретельної оцінки користі/ризику та після розгляду інших варіантів терапії у пацієнтів з обтяженим сімейним анамнезом захворювання аневризмою або у пацієнтів з діагнозом аневризма аорти та/або розшарування аорти, або при наявності факторів ризику, або за умов, що спричиняють аневризму і розшарування аорти (наприклад, синдром Марфана, судинний синдром Елерса-Данлоса, артеріїт Такаясу, гігантоклітинний артеріїт, хвороба Бехчета, артеріальна гіпертензія, встановлений атеросклероз).
У разі виникнення раптового абдомінального болю, болю в грудях або у спині пацієнтам слід порадити негайно звернутися до лікаря у відділення невідкладної допомоги.
Метицилінрезистентний золотистий стафілокок (MRSA)
Імовірно, що метицилінрезистентний золотистий стафілокок має перехресну резистентність до фторхінолонів, зокрема до левофлоксацину. Тому левофлоксацин не рекомендується застосовувати для лікування відомих або підозрюваних MRSA інфекцій, за винятком випадків, коли результати лабораторних тестів підтвердили чутливість збудника до левофлоксацину.
Резистентність E. coli
Резистентність E. сoli, найпоширенішого збудника інфекцій сечових шляхів, до фторхінолонів варіює у різних країнах Європейського Союзу. Під час призначення левофлоксацину лікарям слід враховувати місцеву поширеність резистентності E. coli до фторхінолонів.
Легенева форма сибірської виразки
Клінічна практика базується на дослідженнях чутливості Bacillus anthracis in vitro, а також на експериментальних даних досліджень на тваринах разом з обмеженими даними досліджень за участі людей. Лікарям слід користуватися узгодженими національними та/або міжнародними документами щодо лікування сибірської виразки.
Тендиніт і розрив сухожилля
Тендиніт і розриви сухожилля (не обмежуючись ахіловим сухожиллям), іноді двобічні, можуть виникнути вже протягом 48 годин після початку лікування хінолонами та фторхінолонами і, як повідомлялося, навіть впродовж декількох місяців після припинення лікування у пацієнтів, які отримували добові дози 1000 мг левофлоксацину. Ризик розвитку тендиніту та розриву сухожилля збільшується у пацієнтів літнього віку, пацієнтів із порушеннями функції нирок, пацієнтів із трансплантацією цілісних органів та пацієнтів, які лікувалися одночасно кортикостероїдами. Тому слід уникати одночасного застосування лікарського засобу з кортикостероїдами.
При перших ознаках тендиніту (наприклад, болючий набряк, запалення) лікування слід припинити, а також слід розглянути альтернативне лікування. Пошкоджену кінцівку(и) слід лікувати належним чином (наприклад, забезпечивши іммобілізацію). Кортикостероїди не слід застосовувати у разі виникнення ознак тендинопатії.
Міоклонус
Повідомлялося про випадки міоклонусу у пацієнтів, яким застосовували левофлоксацин (див. розділ «Побічні реакції»). Ризик розвитку міоклонусу підвищується у пацієнтів літнього віку та у пацієнтів з нирковою недостатністю, якщо дозу левофлоксацину не відкориговано відповідно до кліренсу креатиніну. При першій появі міоклонусу левофлоксацин слід негайно відмінити та розпочати необхідне лікування.
Захворювання, спричинені Clostridium difficile
Діарея, особливо тяжка, стійка або з домішками крові упродовж або після лікування левофлоксацином, може бути симптомом хвороби, викликаної Clostridium difficile, найтяжчою формою якої є псевдомембранозний коліт. При підозрі на псевдомембранозний коліт левофлоксацин слід негайно відмінити та одразу розпочати відповідне лікування (наприклад, ванкоміцином). Засоби, що пригнічують моторику кишечнику, протипоказані у цій клінічній ситуації.
Пацієнти зі схильністю до судом
Хінолони можуть знижувати судомний поріг і провокувати розвиток судом. Левофлоксацин протипоказаний пацієнтам з епілепсією в анамнезі.
Як і інші хінолони, лікарський засіб слід з надзвичайною обережністю застосовувати пацієнтам, схильним до судом, наприклад пацієнтам з ураженням центральної нервової системи, при одночасній терапії фенбуфеном та подібними до нього лікарськими засобами або препаратами, які підвищують судомну готовність (знижують судомний поріг), такими як теофілін (див. розділ «Взаємодія з іншими лікарськими засобами та інші види взаємодій»). У випадку появи судом лікування левофлоксацином слід припинити.
Недостатність глюкозо-6-фосфатдегідрогенази
Пацієнти з латентною або розвинутою недостатністю активності глюкозо-6-фосфат- дегідрогенази мають схильність до гемолітичних реакцій при лікуванні хінолоновими антибактеріальними лікарськими засобами, тому таким пацієнтам слід з обережністю застосовувати левофлоксацин через можливість виникнення гемолізу.
Ниркова недостатність
Оскільки левофлоксацин виводиться переважно нирками, для пацієнтів з нирковою недостатністю потрібна корекція дози (див. розділ «Спосіб застосування та дози»).
Реакції підвищеної чутливості
Левофлоксацин може час від часу викликати серйозні потенційно летальні реакції підвищеної чутливості (наприклад, ангіоневротичний набряк, анафілактичний шок), навіть після першого застосування. При виникненні реакцій підвищеної чутливості необхідно припинити прийом левофлоксацину, звернутися до лікаря і розпочати відповідне лікування.
Тяжкі бульозні реакції
При застосуванні левофлоксацину повідомлялося про тяжкі бульозні реакції, такі як синдром Стівенса-Джонсона та токсичний епідермальний некроліз. При виникненні бульозних реакцій необхідно негайно припинити прийом левофлоксацину, звернутися до лікаря і розпочати відповідне лікування.
Зміна рівня глюкози в крові
При застосуванні хінолонів, особливо пацієнтам із цукровим діабетом, які одночасно приймали пероральні гіпоглікемічні засоби (зокрема глібенкламід) або інсулін, повідомлялося про зміни рівня глюкози в крові (гіперглікемія і гіпоглікемія). Спостерігалися випадки гіпоглікемічної коми. Пацієнтам із цукровим діабетом необхідно проводити контроль рівня цукру в крові.
Профілактика реакцій фоточутливості
Повідомлялося про реакції фоточутливості під час лікування левофлоксацином. З метою попередження виникнення реакцій фоточутливості пацієнтам, які приймають левофлоксацин, слід уникати сонячного опромінення та УФ-променів (лампи штучного ультрафіолетового випромінювання, солярій) під час прийому левофлоксацину та протягом 48 годин після припинення застосування левофлоксацину.
У пацієнтів, які застосовують антагоністи вітаміну K, слід контролювати показники згортання крові при одночасному прийомі левофлоксацину та антагоністів вітаміну K (варфарин) через потенційний ризик збільшення показників згортання крові (протромбіновий час/МНВ) та/або кровотечі.
Психотичні реакції
Повідомлялося про виникнення психотичних реакцій у пацієнтів, які отримували хінолони, включаючи левофлоксацин. У дуже рідкісних випадках вони прогресували до суїцидальних думок та самодеструктивної поведінки, іноді лише після прийому єдиної дози левофлоксацину. У випадку, якщо у пацієнта виникають ці реакції, застосування левофлоксацину слід припинити та вдатися до відповідних заходів. Рекомендується з обережністю застосовувати левофлоксацин пацієнтам із психотичними розладами і пацієнтам із психічними захворюваннями в анамнезі.
Подовження інтервалу QT
При прийомі фторхінолонів повідомлялося про випадки подовження інтервалу QT. Слід дотримуватися обережності при застосуванні фторхінолонів, включаючи левофлоксацин, пацієнтам із відомими факторами ризику подовження інтервалу QT:
− синдром вродженого або набутого подовженого інтервалу QT;
− одночасне застосування лікарських засобів, що подовжують інтервал QT (у тому числі антиаритмічних засобів класів ІА і ІІІ, трициклічних антидепресантів, макролідів, антипсихотичних лікарських засобів);
− порушення балансу електролітів (зокрема гіпокаліємія, гіпомагніємія);
− захворювання серця (серцева недостатність, інфаркт міокарда, брадикардія).
Пацієнти літнього віку більш чутливі до лікарських засобів, що подовжують інтервал QT. Тому застосовувати фторхінолони, включаючи левофлоксацин, у цій групі пацієнтів слід з обережністю.
Периферична нейропатія
У пацієнтів, які отримували хінолони та фторхінолони, були зареєстровані випадки сенсорної або сенсомоторної полінейропатії, що призводили до парестезії, гіпестезії, дизестезії або слабкості. У разі виникнення симптомів нейропатії, таких як біль, печіння, поколювання, оніміння або слабкість, пацієнтам, які лікуються препаратом, необхідно поінформувати свого лікаря, аби запобігти розвитку потенційно необоротного стану.
Гепатобіліарні розлади
При застосуванні левофлоксацину повідомлялося про випадки некрозу печінки, аж до печінкової недостатності, що загрожувала життю, переважно у пацієнтів з тяжкими основними захворюваннями, наприклад сепсисом (див. розділ «Побічні реакції»). Пацієнтам слід порекомендувати припинити лікування та звернутися до лікаря, якщо виникають такі прояви хвороби печінки, як анорексія, жовтяниця, темна сеча, свербіж або біль у ділянці живота.
Загострення міастенії гравіс
Фторхінолони, включаючи левофлоксацин, блокують нервово-м’язову передачу і можуть провокувати м’язову слабкість у пацієнтів із міастенією гравіс. При прийомі фторхінолонів у післяреєстраційний період повідомляли про серйозні побічні реакції, включаючи летальні випадки і необхідність підтримки дихання, у пацієнтів із міастенією гравіс. Левофлоксацин не рекомендовано застосовувати пацієнтам із міастенією гравіс в анамнезі.
Порушення зору
Якщо спостерігається порушення зору або інший вплив на очі, слід негайно звернутися до офтальмолога.
Суперінфекція
Застосування левофлоксацину, особливо протягом тривалого часу, може призводити до надмірного зростання нечутливих до дії лікарського засобу мікроорганізмів. Якщо на тлі терапії розвивається суперінфекція, необхідно застосувати належні заходи.
Вплив на лабораторні дослідження
У пацієнтів, які отримували левофлоксацин, визначення опіатів у сечі може дати хибнопозитивний результат. Може виникнути необхідність підтвердити позитивні результати на опіати за допомогою більш специфічних методів.
Левофлоксацин може пригнічувати ріст Mycobacterium tuberculosis, тому можливий хибнонегативний результат при проведенні бактеріологічного дослідження у пацієнтів із туберкульозом.
Розлади з боку крові
Під час лікування левофлоксацином може розвинутися порушення функції кісткового мозку, включаючи лейкопенію, нейтропенію, панцитопенію, гемолітичну анемію, тромбоцитопенію, апластичну анемію або агранулоцитоз (див. розділ «Побічні реакції»). При підозрі на будь-яке з цих порушень слід контролювати результати аналізу крові. У разі отримання аномальних результатів слід розглянути питання щодо припинення лікування левофлоксацином.
Важлива інформація про допоміжні речовини
Цей лікарський засіб містить 860 мг/дозу натрію. Слід бути обережним при застосуванні препарату пацієнтам, які дотримуються натрій-контрольованої дієти.
Застосування у період вагітності або годування груддю.
Через відсутність досліджень і можливе ушкодження хінолонами суглобового хряща в організмі, який росте, лікарський засіб протипоказаний у період вагітності та годування груддю. Якщо під час застосування лікарського засобу настала вагітність, про це слід повідомити лікарю.
Левофлоксацин не зумовлював порушень фертильності або репродуктивної функції у тварин.
Здатність впливати на швидкість реакції при керуванні автотранспортом або іншими механізмами.
Деякі побічні реакції (наприклад, запаморочення/вертиго, сонливість, порушення зору) можуть порушувати здатність пацієнта до концентрації уваги і швидкість його реакції і, таким чином, зумовлювати підвищений ризик у тих ситуаціях, коли ці якості мають особливо велике значення (наприклад, при керуванні автотранспортом або іншими механізмами).
Спосіб застосування та дози.
Дозування залежить від типу та тяжкості інфекції, а також чутливості до лікарського засобу можливого збудника.
Лікарський засіб слід вводити повільно внутрішньовенно 1−2 рази на добу шляхом краплинної інфузії. Тривалість введення 1 флакона левофлоксацину (100 мл розчину для внутрішньовенного введення із 500 мг левофлоксацину) повинна становити не менше 60 хвилин.
Змішування з розчинами для інфузій.
Лікарський засіб сумісний з такими розчинами для інфузій:
0,9 % розчин хлориду натрію, 5 % моногідрат глюкози, 2,5 % декстроза у розчині Рінгера, багатокомпонентні розчини для парентерального харчування (амінокислоти, вуглеводи, електроліти).
Розчин слід використати протягом 3 годин після перфорації флакона.
Лікування левофлоксацином після початкового застосування його внутрішньовенної форми може бути завершене застосуванням пероральної форми за умови прийнятності такого лікування для конкретного пацієнта. Враховуючи біоеквівалентність парентеральних і пероральних лікарських форм, можна застосовувати однакову їх дозу.
Тривалість лікування залежить від перебігу хвороби. Як і при застосуванні інших антибактеріальних засобів, рекомендується продовжувати прийом лікарського засобу принаймні протягом 48−72 годин після нормалізації температури тіла або підтвердженого мікробіологічними тестами знищення збудників.
Дозування для дорослих пацієнтів із нормальною функцією нирок, у яких кліренс креатиніну становить понад 50 мл/хв, наведено у Таблиці 3.
Таблиця 3
Показання | Добова доза, (мг) | Кількість введень на добу | Загальна тривалість лікування1 |
Негоспітальна пневмонія | 500 | 1−2 рази | 7–14 днів |
Ускладнені інфекції сечовивідних шляхів | 500 | 1 раз | 7–14 днів |
Гострий пієлонефрит | 500 | 1 раз | 7–10 днів |
Хронічний бактеріальний простатит | 500 | 1 раз | 28 днів |
Ускладнені інфекції шкіри і м’яких тканин | 500 | 1−2 рази | 7–14 днів |
Легенева форма сибірської виразки | 500 | 1 раз | 8 тижнів |
1 Відповідно до стану пацієнта через кілька днів можливий перехід від початкового внутрішньовенного введення левофлоксацину до перорального застосування з тим самим дозуванням.
Оскільки левофлоксацин виводиться переважно нирками, для хворих із послабленою функцією нирок дозу слід зменшити.
Дозування для дорослих пацієнтів із порушеннями функції нирок, у яких кліренс креатиніну становить менше 50 мл/хв, наведено у Таблиці 4.
Таблиця 4
Кліренс креатиніну, (мл/хв) | Режим дозування (залежно від тяжкості інфекції та нозологічної форми) | ||
250 мг/24 години | 500 мг/24 години | 500 мг/12 годин | |
перша доза: 250 мг | перша доза: 500 мг | перша доза: 500 мг | |
50−20 | наступні: 125 мг/24 години | наступні: 250 мг/24 години | наступні: 250 мг/12 годин |
19−10 | наступні: 125 мг/48 годин | наступні: 125 мг/24 години | наступні: 125 мг/12 годин |
<10 (а також при гемодіалізі та НАПД1) | наступні: 125 мг/48 годин | наступні: 125 мг/24 години | наступні: 125 мг/24 годин |
1 Після гемодіалізу або неперервного амбулаторного перитонеального діалізу (НАПД) додаткові дози не потрібні.
Дозування для пацієнтів із порушеннями функції печінки.
Корекція дози не потрібна, оскільки левофлоксацин незначною мірою метаболізується у печінці та виводиться переважно нирками.
Дозування для пацієнтів літнього віку.
Якщо функції нирок не порушені, немає потреби у корекції дози.
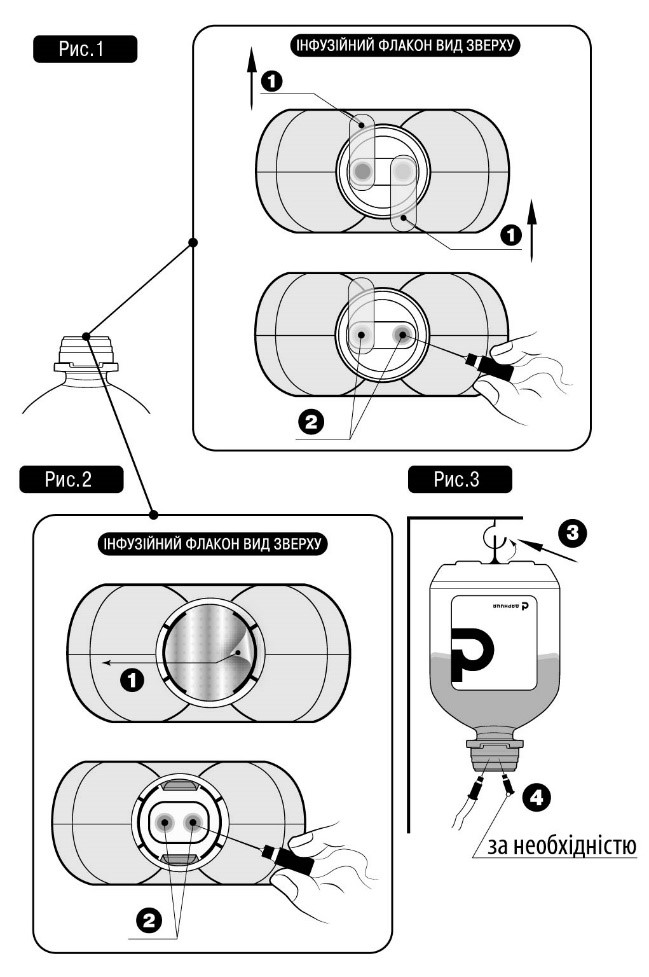
Не вставляти голку(-и) у не передбачені для цього місця полімерного флакона, а тільки у стерильні порти!
Для проведення інфузійного лікування потрібно дотримуватись такого алгоритму:
Зняти захисну пластикову кришку із контролем першого відкриття (якщо така наявна).
Зірвати захисний(-і) клапан(-и) № 1, як показано на рис. 1 та рис.2 (виробник може використовувати різні типи та матеріали для захисних клапанів).
Зняти ковпачок із голки та вставити у будь-який зі спеціальних портів № 2 флакона з інфузійним лікарським засобом (див. рис. 1 та рис. 2).
Інший стерильний порт може використовуватись для введення в інфузійний флакон інших лікарських засобів (№ 4, див. рис. 3), або, у разі недостатньої швидкості потоку для голки-повітровода (№ 4, див. рис. 3).
Підвісити флакон із розчином, використовуючи спеціальне кільце № 3, розташоване на дні флакона (див. рис. 3).
Діти.
Лікарський засіб протипоказаний для застосування дітям, оскільки не виключене ушкодження суглобового хряща.
Передозування.
Симптоми: запаморочення, порушення/сплутаність свідомості, судомні напади, міоклонус, тремор, подовження інтервалу QT.
Лікування. У разі передозування необхідно проводити ретельне спостереження за пацієнтом, включаючи ЕКГ. Лікування симптоматичне. Гемодіаліз, у тому числі перитонеальний діаліз та неперервний амбулаторний перитонеальний діаліз (НАПД), не є ефективним для видалення левофлоксацину з організму. Специфічних антидотів не існує.
Побічні реакції.
Побічні реакції вказані за системами органів та частотою: дуже часто (≥ 1/10), часто (≥ 1/100, <1/10), нечасто (≥ 1/1000, ≤ 1/100), рідко (≥ 1/10000, ≤ 1/1000), дуже рідко (≤ 1/10000), частота невідома (не може бути оцінена на підставі наявних даних).
У кожній групі побічні реакції подано у порядку зменшення їхньої тяжкості.
З боку органів зору*: рідко – порушення зору, таке як затуманений зір; частота невідома – тимчасова втрата зору, увеїт.
З боку органів слуху та вестибулярного апарату*: нечасто – вертиго; рідко – шум у вухах; частота невідома – порушення слуху, втрата слуху.
З боку респіраторної системи, органів грудної клітки та середостіння: нечасто – задишка; частота невідома – бронхоспазм, алергічний пневмоніт.
З боку шлунково-кишкового тракту:часто – діарея, блювання, нудота; нечасто – біль у животі, диспепсія, метеоризм, запор; частота невідома – діарея геморагічна, що може свідчити про ентероколіт, включаючи псевдомембранозний коліт; панкреатит.
З боку печінки і жовчовивідних шляхів: часто – підвищення показників печінкових ензимів (АЛТ/АСТ, лужна фосфатаза, ГГТП); нечасто – підвищення білірубіну в крові; частота невідома – жовтяниця та тяжкі ураження печінки, включаючи випадки розвитку гострої печінкової недостатності, переважно у пацієнтів із тяжкими основними захворюваннями, гепатит.
З боку нирок та сечовидільної системи: нечасто – підвищені показники креатиніну в сироватці крові; частота невідома – гостра ниркова недостатність (наприклад, унаслідок інтерстиціального нефриту).
З боку обміну речовин, метаболізму: нечасто – анорексія; рідко – гіпоглікемія, особливо у пацієнтів, хворих на діабет; частота невідома – гіперглікемія, гіпоглікемічна кома. Ознаками гіпоглікемії можуть бути підвищений апетит, нервовість, підвищене потовиділення, тремтіння кінцівок.
З боку нервової системи*: часто – головний біль, запаморочення; нечасто – сонливість, тремор, дисгевзія; рідко – судоми, парестезії; частота невідома – периферична сенсорна або сенсомоторна нейропатія, порушення тактильних відчуттів, паросмія, включаючи аносмію, дискінезія, екстрапірамідні розлади, інші порушення координації рухів, у тому числі при ходьбі, заклякання, агевзія, непритомність, доброякісна внутрішньочерепна гіпертензія, міоклонус.
З боку психіки*: часто – безсоння; нечасто – тривожність, сплутаність свідомості, дратівливість, неспокій; рідко – психотичні розлади (зокрема галюцинації, параноя), депресія, ажитація, патологічні сновидіння, нічні жахи, стан страху; частота невідома – психотичні розлади зі самодеструктивною поведінкою, включаючи суїцидальну спрямованість мислення або дій, манія.
З боку серцево-судинної системи: рідко – тахікардія, відчуття серцебиття; частота невідома – шлуночкова тахікардія, що може призводити до зупинки серця; шлуночкова аритмія та аритмія типу torsade de pointes (переважно у пацієнтів із факторами ризику подовження інтервалу QT), подовження інтервалу QT на ЕКГ, артеріальна гіпотензія, колапс, васкуліт, флебіт.
З боку крові та лімфатичної системи: нечасто – лейкопенія, еозинофілія; рідко – нейтропенія, тромбоцитопенія, яка спричиняє підвищену схильність до крововиливів або кровотеч; частота невідома – порушення функції кісткового мозку, включаючи апластичну анемію, панцитопенію, агранулоцитоз, гемолітичну анемію.
З боку імунної системи: рідко – ангіоневротичний набряк, реакції підвищеної чутливості, включаючи анафілактичний шок, анафілактоїдний шок (анафілактичні та анафілактоїдні реакції іноді можуть виникати навіть після застосування першої дози).
З боку шкіри та підшкірної клітковини: нечасто – висипання, свербіж, кропив’янка, почервоніння шкіри, гіпергідроз; частота невідома – токсичний епідермальний некроліз, синдром Стівенса-Джонсона, ексудативна мультиформна еритема, реакції фоточутливості, підвищена чутливість до сонячного та ультрафіолетового випромінювання, лейкоцитопластичний васкуліт, стоматит, гіперпігментація шкіри.
З боку опорно-рухової системи та сполучної тканини*: нечасто – артралгія, міалгія; рідко – ураження сухожиль, у тому числі тендиніт (наприклад, ахіллового сухожилля), м’язова слабкість, яка може мати особливе значення для хворих на тяжку міастенію gravis; частота невідома – рабдоміоліз, розрив сухожилля, зв’язок, м’язів, артрит.
Інфекції та інвазії: нечасто – грибкові інфекції, включаючи гриби роду Candida, резистентність патогенних мікроорганізмів.
Загальні розлади та реакції у місці введення*: часто – реакція у місці введення, включаючи почервоніння та біль; нечасто – астенія; рідко – підвищення температури тіла; частота невідома – загальна слабкість, біль (включаючи біль у спині, грудях та кінцівках); як і при застосуванні інших фторхінолонів, можливі напади порфірії у пацієнтів із порфірією.
* У дуже рідкісних випадках у пацієнтів, які отримували хінолони та фторхінолони, незалежно від наявних факторів ризику повідомляли про тривалі (протягом місяців або років), інвалідизуючі та потенційно незворотні серйозні побічні реакції, які впливають на різні, а іноді на декілька відразу, системи організму та органи чуття (у тому числі реакції, такі як тендиніт, розрив сухожилля, артралгія, біль у кінцівках, порушення ходи, невропатія, пов’язана з парестезією, депресія, втома, порушення пам’яті, порушення сну, порушення слуху, зору, смаку та запаху).
Повідомлення про підозрювані побічні реакції.
Повідомлення про підозрювані побічні реакції після реєстрації лікарського засобу є важливою процедурою. Це дозволяє продовжувати моніторинг співвідношення «користь/ризик» для відповідного лікарського засобу. Медичним працівникам необхідно повідомляти про будь-які підозрювані побічні реакції через національну систему повідомлень.
Термін придатності. 3 роки.
Умови зберігання.
Зберігати в оригінальній упаковці при температурі не вище 25 °С. Не заморожувати.
Зберігати у недоступному для дітей місці.
Несумісність.
Розчин не слід змішувати з гепарином або лужними розчинами (наприклад, із гідрокарбонатом натрію), з іншими лікарськими засобами.
Упаковка.
По 100 мл у флаконі; по 1 флакону в пачці; по 100 мл у флаконах.
Категорія відпуску.
За рецептом.
Виробник. ПрАТ «Фармацевтична фірма «Дарниця».
Місцезнаходження виробника та адреса місця провадження його діяльності.
Україна, 02093, м. Київ, вул. Бориспiльська, 13.